Chronic kidney disease (CKD) patients are subject to a wide variety of pathophysiologic processes that challenge the structural and functional integrity of both central and peripheral nervous systems. Neurologic dysfunction can be episodic or chronic and can reflect a wide range of humoral, metabolic, inflammatory, and vascular insults. These may be attendant to the underlying conditions that have led to end stage kidney disease (ESKD), advanced uremia itself, or to the dialysis procedure (on a variety of levels). The integrated product of these factors contributes to neurocognitive performance, depression, health-related quality of life, and the ability of the patient to tolerate the dialysis procedure whilst leading a full and independent life in the hours spent not actually receiving dialysis. This chapter is limited to discussion of the brain and peripheral nervous system, and encompasses sleep disorders and combination pathologies such as restless legs syndrome.
I. CENTRAL NERVOUS SYSTEM. When considering dysfunction of the central nervous system (CNS) in the dialyzed uremic patient, it’s important to consider the range of structural abnormalities that can occur, as well as the impact of the uremic milieu. Many of these considerations are often present together and may result in compound effects.
A. Intracranial bleeding and ischemic stroke. Spontaneous subdural hemorrhage is common. The rate has been increasing over recent years, possibly associated with increased use of anticoagulation in patients with atrial fibrillation in an attempt to reduce the risk of stroke. Intracranial or subarachnoid bleeds are not uncommon (even during the dialysis procedure itself). They are a particular problem in patients with polycystic kidneys who may have intracranial aneurysms. Headache occurs in both disequilibrium and early cerebral hemorrhage, but the pattern of recovery is different and new onset headache may need to be investigated for possible intracranial bleeding by CT or MRI (embracing the limitations of contrast use in this population). Heparin-free dialysis should be used. Both ischemic and hemorrhagic strokes are common and catastrophic events, but usually present little diagnostic challenge. Both short- and long-term management are controversial with there being very little data relating to the application of intracerebral thrombolysis or primary/secondary preventative measures in hemodialysis patients. The efficacy and safety profile of all of these interventions may very well be very different in dialysis patients compared with the general population, where they were developed.
B. Subclinical brain structural abnormalities. There are several pathologies detectable by brain MRI in the brain of dialysis patients. These may be entirely asymptomatic or linked to more subtle defects in neurocognitive function, often only apparent on specific testing. They are often progressive. Many of these changes do not appear to be associated with classical cardiovascular risk factors, and instead seem to be predominantly driven by other factors such as microvascular disease, inflammation, and challenged perfusion (both in general and episodically during hemodialysis). These abnormalities range from silent cerebral infarct to changes both in the white matter (leukoaraiosis) and grey matter (cortical atrophy).
1. Silent cerebral infarcts. Nakatani and coworkers examined the hypothesis that hemodialysis patients develop silent cerebral infarcts (SCI). These silent infarcts are mainly subcortical and lacunar without causing any neurologic deficit, but are thought to be a risk factor for developing symptomatic infarct or hemorrhagic strokes. Nakatani and coworkers (2003) examined a group of 50 hemodialysis patients and found that in those who developed SCI, associated risk factors were smoking, lower HDL cholesterol, higher uric acid levels, and higher levels of hepatocyte growth factor. Echocardiographically, the group who developed SCI had higher interventricular septal thickness at the end of diastole, higher posterior wall thickness at the end of diastole, and higher left ventricular mass index. On 24-hour blood pressure monitoring, the group with silent infarcts was not more hypertensive in general, but did not evidence the healthy pattern of a nocturnal fall in blood pressure. One possible mechanism in the causation of SCI might be microbubbles generated during the hemodialysis procedure and undetected by the air alarms may find their ways into the cerebral circulation and cause ischemic damage (Forsberg, 2010).
2. Cerebral atrophy. Cerebral (cortical) atrophy has been identified in hemodialysis patients through both CT and MRIbased studies. The degree of cerebral atrophy is associated with duration of dialysis. Cerebral blood flow is lower in between dialysis sessions and higher during hemodialysis. These hemodynamic changes and changes in cerebral oxygenation are less pronounced in peritoneal dialysis patients, suggesting that there may be iatrogenic cerebral effects of hemodialysis (Prohovnik, 2007).
3. Leukoaraiosis. Leukoaraiosis describes nonspecific changes in the brain white matter caused by loss of axons and myelin. This is usually associated with ischemic injury. The MRI appearance is that of high signal intensity on T2-weighted images. Leukoaraiosis is a risk factor for developing dementia, mobility problems, and strokes, and has been described in the literature primarily as an age-related phenomenon. In the non-CKD population, leukoaraiosis is associated with reduction in cognitive function and with increased prevalence and severity of depression.
Several studies have identified this pattern of structural brain injury as being common in hemodialysis patients; in fact, a universal finding after only 3 months of hemodialysis. The severity of reduction in cognitive function was proportional to the distribution and amount of white matter injury, and in turn this was proportional to the degree of cardiovascular instability during hemodialysis sessions (Eldehini, 2014).
C. Humoral abnormalities influencing brain function
1. Uremic encephalopathy. Encephalopathy is a cardinal feature of untreated uremia. Initial manifestations are subtle: flattened affect, irritability, and poor rapport with others. Formal evaluation at this stage may reveal patchy cognitive or psychomotor behavior. Event-related brain potentials (stimulus-evoked averaged electroencephalogram [EEG] waveforms) may be abnormal. As uremia advances, lassitude gives way to disorientation, confusion, delirium, stupor, and, preterminally, coma. There are accompanying motor disturbances: tremulousness, myoclonus, and asterixis (flapping tremor). These major signs of uremic encephalopathy will reliably regress within a week or so of initiation of regular dialysis; failure to do so should lead to an alternative or additional diagnosis.
2. Metabolic and electrolytic causes. Hypercalcemia from any cause (often relating to CKD mineral bone disorder or its treatments) can present as an acute confusional state or coma. Severe low or high serum sodium levels can also result in a predominantly neurologic presentation. The presence of cerebral atrophy often makes the dialysis patient remarkably resistant to the development of severe cerebral edema as a result of abnormal tonicity. Hypoglycemia may present in diabetic patients due to inappropriate hypoglycemic therapy, or to further reductions in residual renal function with reduced insulin metabolism. In nondiabetic patients hypoglycemia may occur as a result of reflex hyperinsulinemia after exposure to hemodialysis solutions containing higher glucose concentrations, or as a hypoglycemic response to glucose-free dialysate.
Acute aluminum intoxication can present with an acute neurotoxicity syndrome characterized by agitation, confusion, seizures, myoclonic jerks, and coma. This is quite uncommon now compared with the bygone era when there were less stringent water treatment standards and heavy reliance on aluminum-containing salts for oral binding of phosphate. Still, even today, the acute syndrome can be seen when dialysis solution becomes highly contaminated with aluminum for some reason, or in the course of deferoxamine therapy. In this setting, the plasma aluminum level is usually more than 500 mcg/L (19 mcmol/L), and typical EEG changes (multifocal bursts of slow or delta wave activity, often accompanied by spikes) are present. More information about aluminum toxicity is given in Chapter 36 on mineral bone disorders.
3. Infection and inflammation. Both systemic and local infection and inflammation can affect the brain in dialysis patients. Sepsis in this patient group not uncommonly presents without a typical pyrexial response (especially in the elderly), and the initial manifestation can be central obtundation. Dialysis patients are immunosuppressed both as a consequence of the uremic state and of immunomodulatory therapy given as part of treatment of their underlying disease. They also are at higher risk of a wide range of encephalitic or meningitic processes, especially those with more “slow burning” presentations such as tuberculous meningitis.
Endotoxemia is another important factor that could be implicated in the pathogenesis of hemodialysis-induced brain injury. Endotoxemia is well described in CKD5D patients, and it induces a systemic proinflammatory state (McIntyre, 2011). These patients suffer gut hypoperfusion and increased bowel permeability, resulting in bacterial and endotoxin translocation to the circulation. The level of resultant circulatory stress is associated with the severity of endotoxemia. Hemodialysis patients are in a chronic state of endotoxemia, with acute exacerbations from recurrent mesenteric ischemia accompanying each hemodialysis session. The repeated endotoxemic insult may also aggravate the effects of hemodialysis on cerebral perfusion with secondary ischemic white matter subcortical brain injury.
D. Acute episodic dysfunction
1. Disequilibrium syndrome. Rapid correction of advanced uremia is sometimes complicated by a characteristic syndrome of neurologic dysfunction appearing in the last part of dialysis or shortly afterward. Hemodialysis is usually involved, but disequilibrium can also occur with peritoneal dialysis. In its mildest form, the syndrome is limited to restlessness, headache, nausea, and vomiting; more severe manifestations include confusion and major seizures. The syndrome is believed to be caused by brain swelling due to a lag in osmolar shifts between blood and brain during dialysis, but changes in brain pH may also play a role. Disequilibrium occurs in a major form in previously undialyzed patients, but minor features may complicate chronic therapy. Disequilibrium is more likely to occur when patients with advanced states of uremia are dialyzed for excessive lengths of time during their first treatment sessions, especially in the era of using higher-efficiency dialyzers in this setting. The initial dialyses should be relatively short, so as to reduce elevated serum urea levels slowly over the course of several days. The routine use of anticonvulsants in this setting should be avoided.
2. Other factors effecting tonicity. Rapid shifting of other osmotically active substances (glucose and sodium) may also contribute to presentation with acute obtundation, and further consideration may need to be given to glucose level correction and careful individualization of dialysate conductivity to minimize these additional insults.
3. Dialysis-induced reduction in cerebral perfusion/oxygenation. Failure to maintain blood pressure during dialysis may also precipitate an acute reduction in consciousness levels. Diagnosis and management of intradialytic hypotension is dealt with in more detail in other sections of this handbook, but immediate recognition and corrective measures are essential to restore normal functioning and reduce the risk of a watershed area cerebral infarct. Such episodes may also be important in driving chronic subclinical white matter injury.
4. Coning. Uncal and cerebellar tonsillar herniation can occur without other coexisting pathologic lesions. This can present with a severe dialysis-induced headache and a reduced level of consciousness, and result in death. More commonly, this presentation occurs in the setting of either inherited abnormalities predisposing to coning (such as the so-called Chiari malformation, where there is partial hindbrain herniation through the foramen magnum, sometimes seen in spina bifida) or after neurosurgery. Cerebrospinal fluid diversion and, in particular, shunt malfunction can also increase the risk of dialysis-induced brainstem herniation. Limitation of ultrafiltration rate and careful matching of dialysate tonicity to plasma are the essentials of management in this setting.
5. Nonconvulsivestatus epilepticus.Status epilepticus may present with confusion or more severe reductions in the level of consciousness. When occurring without obvious convulsive activity (Iftikhar, 2007), it may mimic collapse from either a catastrophic intracerebral event (although with normal brain imaging) or acute cardiovascular insufficiency.
Typically, the EEG in nonconvulsive status epilepticus shows generalized spike-and-wave complexes at 3 Hz or repetitive generalized or focal spikes, sharp-waves, and spikeand-wave complexes at > 4/sec. Events that can precipitate nonconvulsive status include alcohol, drug withdrawal, infection, hypoxia, cerebrovascular accident, menstruation, cyclosporine A therapy, malignancy, and antibiotic neurotoxicity. Antibiotics which have been reported to cause seizures in patients with decreased renal function, include penicillins, cephalosporins, imipenem/cilastatin, and quinolones. Management is focused on dealing with precipitating causes and use of standard anticonvulsant drugs for the management of acute epilepsy.
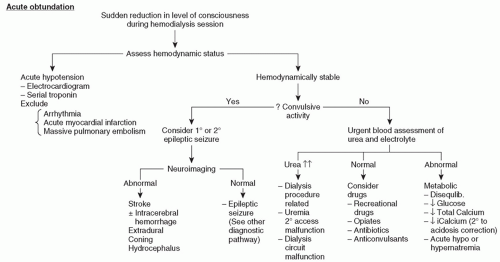
E. Differential diagnosis of acute obtundation syndrome, dialysis disequilibrium, and chronic dementia. The differential diagnosis for each of these conditions is large. A partial list to consider when confronted with a patient with acute obtundation is given in Table 40.1. Mimics of dialysis disequilibrium are given in Table 40.2, and those for chronic dementia in Table 40.3. Proposed management strategies for acute obtundation are shown in Figure 40.1 and for chronic obtundation in Figure 40.2.
F. Diagnosis and management of epileptic seizures
1. Etiology. Seizures are not uncommon in dialysis patients. Generalized seizures are an integral feature of advanced uremic encephalopathy. Seizures can also be a manifestation of severe disequilibrium syndrome, as discussed above. Table 40.4 lists the most common associated conditions. Intracranial hemorrhage commonly leads to focal seizures, while most of the other causes lead to generalized seizures.
Seizures characterize both aluminum-induced encephalopathy and severe hypertension. In children with renal failure, the incidence of seizures is higher than in adults. Predialysis hypocalcemia can result in seizures during or soon after dialysis because of the fall in serum ionized calcium level associated with rapid correction of acidosis. As in any patient with hypocalcemia, associated (and often causal) hypomagnesemia should be excluded. Hypoglycemia can occur if glucose-free dialysis solution is used.
TABLE 40.1 Partial Differential Diagnoses of Acute Obtundation in Maintenance Dialysis patients
Uremic encephalopathy
Drug intoxication (by drugs renally excreted)
Antibiotics
Antiviral agents
Opiates
Anticonvulsants
Central nervous system infection
Meningitis
Encephalitis
Endocarditis
Hypertensive encephalopathy
Hemorrhage
Subarachnoid
Subdural
Intracranial
Acute aluminum toxicity (coingestion of citrate, highly contaminated dialysate)
Wernicke’s encephalopathy (in patients with vomiting, poor food intake)
TABLE 40.2 Conditions That May Mimic Dialysis Disequilibrium Syndrome
Intracranial bleeding
Subdural
Subarachnoid
Intracranial
Metabolic disorders
Hyperosmolar states
Hypercalcemia
Hypoglycemia
Hyponatremia
Cerebral infarction
Hypotension
Excessive ultrafiltration
Cardiac arrhythmia
Myocardial infarction
Anaphylaxis
Aluminum intoxication (subacute)
TABLE 40.3 Partial Differential Diagnoses of Chronic Dementia in Dialysis Patients
Idiopathic presenile dementia
Vascular dementia
Depression
Chronic subdural hematoma
Drug intoxication
Metabolic disorders
Hypercalcemia (autonomous hyperparathyroidism or iatrogenic)
Hypoglycemic brain damage
Demyelination syndrome secondary to hyponatremia
Uremia (underdialysis)
Hydrocephalus (possibly secondary to subarachnoid hemorrhage)
Seizures tend to be more common in patients taking a variety of “epileptogenic” drugs. Penicillins and cephalosporins are common offenders, especially if high doses are given or when provision for dose reduction in the setting of CKD has not been made. A selection of other epileptogenic drugs is given in Table 40.4. A variety of poisonings in dialysis patients can also present with seizures, including star fruit ingestion (numbness, weakness, obtundation, seizures). Some anticonvulsant drugs may have enhanced removal by high-efficiency hemodialysis (e.g., carbamazepine) and this may result in precipitation of seizures due to reduction of drug plasma levels below the therapeutic threshold.
FIGURE 40.1 Evaluation and Management of Acute Obtundation.
Only gold members can continue reading. Log In or Register to continue