Chapter 20 Neoplasia
Alkylators








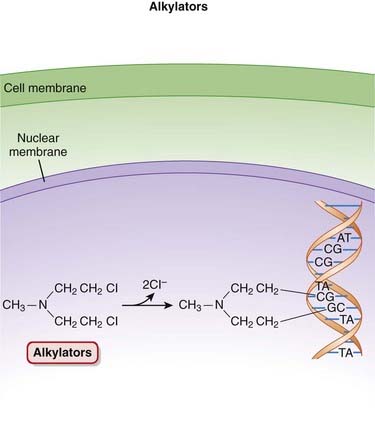
MOA (Mechanism of Action)
 The alkylating agents transfer alkyl (chemical) groups to DNA. DNA alkylation in the nucleus leads to the death of the cell.
The alkylating agents transfer alkyl (chemical) groups to DNA. DNA alkylation in the nucleus leads to the death of the cell.


 Alkylating agents are considered to be cell cycle phase nonspecific, with cells in G1 and S phases being most susceptible (Figure 20-1).
Alkylating agents are considered to be cell cycle phase nonspecific, with cells in G1 and S phases being most susceptible (Figure 20-1).







Pharmacokinetics
 Oral dosage forms are available for cyclophosphamide, melphalan, chlorambucil, and busulfan. Lomustine is available only in oral dosage forms. The rest are all intravenous.
Oral dosage forms are available for cyclophosphamide, melphalan, chlorambucil, and busulfan. Lomustine is available only in oral dosage forms. The rest are all intravenous.

























Side Effects
 Nausea, vomiting: These are common side effects with cytotoxic agents, which tend to target rapidly dividing cells, including those of the GI tract.
Nausea, vomiting: These are common side effects with cytotoxic agents, which tend to target rapidly dividing cells, including those of the GI tract.






Important Notes
 A number of the alkylating agents (cyclophosphamide, ifosfamide, estramustine, melphalan, and chlorambucil) are also known as nitrogen mustards. These agents are related to mustard gas, a biologic warfare agent used during World War I.
A number of the alkylating agents (cyclophosphamide, ifosfamide, estramustine, melphalan, and chlorambucil) are also known as nitrogen mustards. These agents are related to mustard gas, a biologic warfare agent used during World War I.





Anthracyclines


MOA (Mechanism of Action)


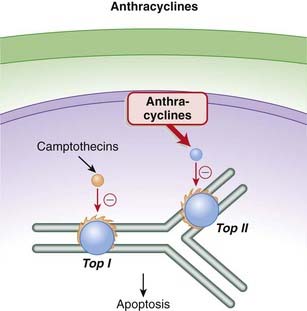
 The anthracyclines prevent the resealing step from occurring by intercalating into and inhibiting the DNA–topoisomerase II complex after the nicking phase. This results in a large number of DNA fragments, eventually prompting the cancer cell to undergo apoptosis (Figure 20-2).
The anthracyclines prevent the resealing step from occurring by intercalating into and inhibiting the DNA–topoisomerase II complex after the nicking phase. This results in a large number of DNA fragments, eventually prompting the cancer cell to undergo apoptosis (Figure 20-2).























Contraindications
 Severe cardiac disease: Anthracyclines should be used only with extreme caution and after a careful risk-benefit assessment in these patients. See Side Effects.
Severe cardiac disease: Anthracyclines should be used only with extreme caution and after a careful risk-benefit assessment in these patients. See Side Effects.
Side Effects
 Nausea and vomiting are common side effect with cytotoxic agents, which tend to target rapidly dividing cells, including those of the GI tract.
Nausea and vomiting are common side effect with cytotoxic agents, which tend to target rapidly dividing cells, including those of the GI tract.


Serious
 Cardiotoxicity: The free radicals generated by the anthracyclines cause peroxidation of the cardiac sarcoplasmic reticulum, leading to a Ca2+-dependent cardiac necrosis. The reason this toxicity is selective for cardiac tissue is that catalase, able to neutralize these free radicals, is not found in cardiac tissue.
Cardiotoxicity: The free radicals generated by the anthracyclines cause peroxidation of the cardiac sarcoplasmic reticulum, leading to a Ca2+-dependent cardiac necrosis. The reason this toxicity is selective for cardiac tissue is that catalase, able to neutralize these free radicals, is not found in cardiac tissue.
Important Notes
 Cardiotoxicity associated with anthracyclines can occur both acutely and chronically. Acute toxicity is characterized by abnormal electrocardiograms (ECGs) and reductions in systolic function. Chronic toxicity is cumulative and dose related. It manifests as congestive heart failure, and once it has reached this point it has a very high mortality rate. This chronic cardiotoxicity is of greater concern, and it is addressed using a number of strategies, including limitations on doses used, as well as use of liposomal formulations and adjuvant agents, as described later.
Cardiotoxicity associated with anthracyclines can occur both acutely and chronically. Acute toxicity is characterized by abnormal electrocardiograms (ECGs) and reductions in systolic function. Chronic toxicity is cumulative and dose related. It manifests as congestive heart failure, and once it has reached this point it has a very high mortality rate. This chronic cardiotoxicity is of greater concern, and it is addressed using a number of strategies, including limitations on doses used, as well as use of liposomal formulations and adjuvant agents, as described later.
Advanced
 Strategies to minimize cardiotoxicity include the use of a cardioprotective drug such as dexrazoxane. The generation of free radicals by anthracyclines is iron dependent. Dexrazoxane chelates iron that is bound in anthracycline complexes, and this prevents the formation of the free radicals that damage the myocardium. Dexrazoxane does not appear to impair the antitumor activity of the anthracyclines.
Strategies to minimize cardiotoxicity include the use of a cardioprotective drug such as dexrazoxane. The generation of free radicals by anthracyclines is iron dependent. Dexrazoxane chelates iron that is bound in anthracycline complexes, and this prevents the formation of the free radicals that damage the myocardium. Dexrazoxane does not appear to impair the antitumor activity of the anthracyclines.Drug Interactions
 It appears that the cardiotoxic effects of anthracyclines may be worsened by concurrent administration of trastuzumab. Trastuzumab is a monoclonal antibody that is used in the treatment of breast cancers expressing the HER2/neu receptor. A number of anthracyclines are used in treating breast cancer.
It appears that the cardiotoxic effects of anthracyclines may be worsened by concurrent administration of trastuzumab. Trastuzumab is a monoclonal antibody that is used in the treatment of breast cancers expressing the HER2/neu receptor. A number of anthracyclines are used in treating breast cancer.
Antimetabolites





MOA (Mechanism of Action)
Folate Analogues
 Tetrahydrofolate (THF) is an essential cofactor in the transformation of 2’-deoxyuridylate (dUMP) to 2’-deoxythymidylate (dTMP). This is a required step in the synthesis of purines and thus DNA.
Tetrahydrofolate (THF) is an essential cofactor in the transformation of 2’-deoxyuridylate (dUMP) to 2’-deoxythymidylate (dTMP). This is a required step in the synthesis of purines and thus DNA. THF is synthesized by the actions of dihydrofolate reductase (DHFR). Methotrexate has a high affinity for DHFR and competitively inhibits DHFR (Figure 20-3).
THF is synthesized by the actions of dihydrofolate reductase (DHFR). Methotrexate has a high affinity for DHFR and competitively inhibits DHFR (Figure 20-3).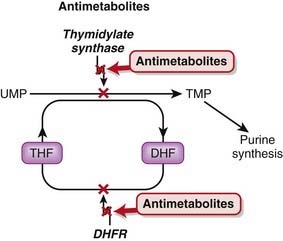




Pyrimidine Analogues
 Fluorouracil is a uracil analogue. It is converted to FdUMP (fluorodeoxyuridine monophosphate) and although it interacts with thymidylate synthetase, it cannot be converted to dTMP because of the fluoro component and therefore results in a deficiency of dTMP. Without dTMP, DNA synthesis cannot occur. It is considered to be a fraudulent nucleotide.
Fluorouracil is a uracil analogue. It is converted to FdUMP (fluorodeoxyuridine monophosphate) and although it interacts with thymidylate synthetase, it cannot be converted to dTMP because of the fluoro component and therefore results in a deficiency of dTMP. Without dTMP, DNA synthesis cannot occur. It is considered to be a fraudulent nucleotide.






Pharmacokinetics
 Methotrexate can be administered orally, intravenously, intramuscularly, or intrathecally. It is not able to cross the blood-brain barrier, so entry into the central nervous system (CNS) can be achieved only by intrathecal administration.
Methotrexate can be administered orally, intravenously, intramuscularly, or intrathecally. It is not able to cross the blood-brain barrier, so entry into the central nervous system (CNS) can be achieved only by intrathecal administration.


















Side Effects
Folate Analogues
 Myelosuppression: Conventional chemotherapy agents work by targeting rapidly dividing cells. This nonspecific effect can also target rapidly dividing cells in other areas of the body, including bone marrow and the GI tract.
Myelosuppression: Conventional chemotherapy agents work by targeting rapidly dividing cells. This nonspecific effect can also target rapidly dividing cells in other areas of the body, including bone marrow and the GI tract.









Purine Analogues
 Myelosuppression develops more gradually than with the folate analogues. It tends to be worse with thioguanine.
Myelosuppression develops more gradually than with the folate analogues. It tends to be worse with thioguanine.








Important Notes
 High-dose regimens of methotrexate may require rescue with folinic acid, also known as leucovorin. Folinic acid is a reduced form of folic acid. Methotrexate is an “antifolate” drug, and patients who are taking high doses or receiving chronic therapy are likely to experience severe symptoms of folate deficiency unless they are treated adjunctively with leucovorin.
High-dose regimens of methotrexate may require rescue with folinic acid, also known as leucovorin. Folinic acid is a reduced form of folic acid. Methotrexate is an “antifolate” drug, and patients who are taking high doses or receiving chronic therapy are likely to experience severe symptoms of folate deficiency unless they are treated adjunctively with leucovorin.

Advanced
Pharmacogenetics
 Thiopurine methyltransferase (TPMT) plays a role in the metabolic inactivation of mercaptopurine. Approximately 15% of Caucasians have reduced activity of this enzyme, and these individuals are at greater risk for toxicity. TPMT genotyping is now readily available, and genotype-based dosage recommendations are available.
Thiopurine methyltransferase (TPMT) plays a role in the metabolic inactivation of mercaptopurine. Approximately 15% of Caucasians have reduced activity of this enzyme, and these individuals are at greater risk for toxicity. TPMT genotyping is now readily available, and genotype-based dosage recommendations are available.




