Nausea and Vomiting
LEARNING OBJECTIVES
• ETIOLOGY
Nausea and/or vomiting is a common presentation in ambulatory and urgent care centers, serving as the chief complaint in 3.7% of emergency room visits. While most causes are self-limiting, it can be a symptom of a variety of diseases throughout the body, many of which are serious or life threatening, affecting the central nervous system, genitourinary tract, gastrointestinal and surrounding organ systems. In addition, nausea and vomiting can be caused by medications, toxins, cardiovascular disease, and metabolic diseases. Causes can be iatrogenic, infectious, inflammatory, and mechanical in nature. Given the broad variety of causes and the potential for involvement of multiple organ systems, a very careful and comprehensive history and physical examination are essential.
• DIAGNOSIS
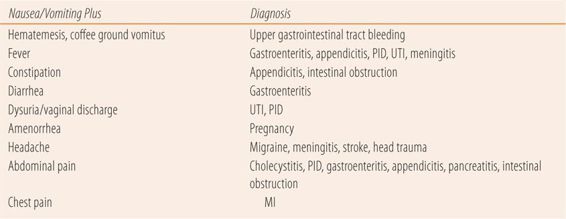
Because of the broad range of diagnostic possibilities, the key to identifying the cause of nausea and/or vomiting lies with the associated symptoms (Table 11.1). For example, gastroenteritis typically presents with a sudden onset, a history of exposure to potentially tainted foods, or others with similar symptoms. Most patients concurrently complain of abdominal discomfort, fever and diarrhea. Diagnostic accuracy is dependent on a careful history and physical examination, since there are few laboratory tests involving the gastrointestinal tract that can specifically diagnose the cause of nausea and vomiting. Laboratory tests and imaging studies are used primarily in diagnosing those causes not related to the stomach or intestines.
| TABLE 11.1 | Associated Symptoms–Based Differential Diagnosis of Nausea and Vomiting |
• COMMON CAUSES OF NAUSEA AND/OR VOMITING
Gastroenteritis
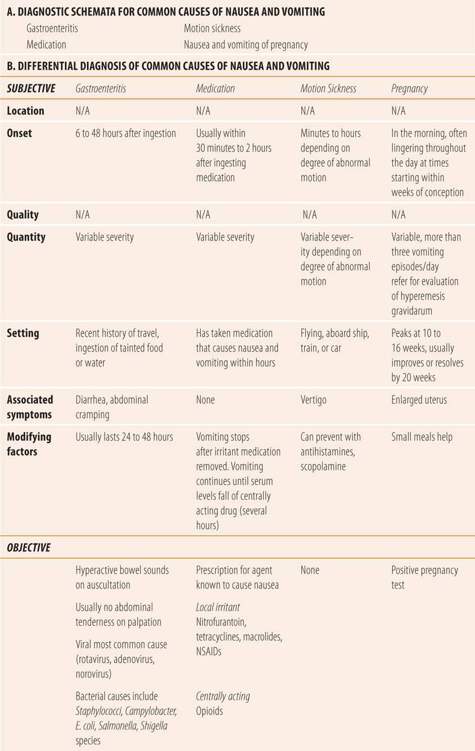
Gastroenteritis can be caused by both viral and bacterial pathogens (Table 11.2). Common viral gastroenteritis pathogens include rotavirus, norovirus, and adenovirus. Bacterial gastroenteritis pathogens include Staphylococci, Campylobacter, E. coli, Shigella and Salmonella species. Onset can occur hours to days after ingestion and the nausea and vomiting usually subsides within 24 to 48 hours. Patients with nausea and vomiting lasting more than 48 hours should be referred. The nausea and vomiting may occur alone but is usually accompanied by diarrhea, fever, cramping abdominal pain, and malaise. Usually patients have a history of recent travel, a sick family member, or recent attendance at a potluck, picnic, or other potential source of spoiled food. Physical examination is negative for abdominal tenderness and bowel sounds are hyperactive on auscultation.
| TABLE 11.2 | Common Causes of Nausea and Vomiting |
Medication
Medication is another common cause of nausea and vomiting. Drugs can be local irritants, stimulate specific centers in the brain such as the chemoreceptor trigger zone, or have both mechanisms of inducing emesis. Tetracyclines, nitrofurantoin, macrolide antibiotics, and NSAIDs are common causes of drug-induced irritant nausea and vomiting. Patients have a history of very recent ingestion of the offending agent, and the nausea and vomiting are frequently preceded or accompanied by abdominal discomfort or pain. The initial episode of emesis usually provides relief by removing the medication from the stomach. The incidence of this type of reaction can be reduced by taking the medication with food and/or a full glass of water. Opioids are by far the most common cause of drug-induced centrally mediated vomiting. The symptoms begin as soon as the serum level of the medication is high enough to stimulate the chemoreceptor trigger zone in the brain and continue for hours until the serum levels fall drastically. Vertigo may precede or accompany the nausea and vomiting. This type of nausea can only be prevented by medication such as phenothiazines, which block the effects of the drug on the chemoreceptor trigger zone. Taking narcotics with food or a full class of water has no impact on the incidence or duration of drug-induced central nausea and vomiting. Cancer chemotherapy agents cause nausea and vomiting by both mechanisms.
Motion Sickness
In susceptible patients, flying, traveling by ship, or traveling in any moving vehicle such as a train or automobile can cause stimulation of the vestibular apparatus of the inner ear, inducing vertigo, nausea, and eventually emesis. The more severe and disorienting the motion the patient experiences, the more likely the patient will develop motion sickness. The incidence of motion sickness can be reduced by using agents that stabilize the vestibular apparatus such as meclizine, diphenhydramine, and scopolamine.
Nausea and Vomiting of Pregnancy
Seventy to eighty percent of pregnant women will experience “morning sickness” in the first trimester of pregnancy. The term morning sickness is a misnomer since the majority of women who experience it will have the uncomfortable sensations throughout the day. Onset occurs within weeks of conception, peaking at 10 to 16 weeks and resolving by 20 weeks. While the exact cause of the nausea and vomiting of pregnancy is unclear, both human chorionic gonadotropin (hCG) and rising estrogen levels have been implicated. Hyperemesis gravidarum is a condition of severe nausea and vomiting during pregnancy that can lead to excess maternal and fetal morbidity and mortality. Pregnant women who experience three or more episodes of vomiting per day should be quickly referred for definitive diagnosis and treatment. All females of childbearing age who present with nausea and vomiting should be questioned about their last menstrual period (LMP) and have a pregnancy test done.
• POTENTIALLY SERIOUS CAUSES OF NAUSEA AND VOMITING
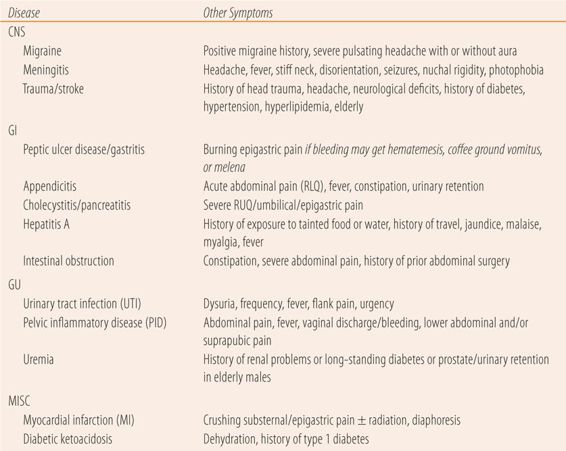
All patients who present with nausea and vomiting should be screened for the following potentially serious causes (Table 11.3). A careful history and, if possible, physical examination are needed to determine the need for immediate referral. In a community pharmacy, the patient’s profile can be quickly reviewed for medications and diagnoses, plus a modified review of systems covering each potential cause can be quickly done.
| TABLE 11.3 | Typical Presentation of Serious Causes of Nausea and Vomiting |
Migraine Headache
The vast majority of patients with migraines experience nausea with or without vomiting. Check for the presence of a pulsating headache, photophobia, phonophobia, aura, or a history of migraine or other vascular headaches. See Chapter 13 for further details.
Trauma/Stroke (CVA)
Patients with a severe headache, recent history of head trauma, a sudden change in vision, or other neurological deficits should be immediately referred. See Chapter 13 for further details.
Meningitis
In addition to nausea and vomiting, patients with meningitis may present with high fever, headache, disorientation, a stiff neck (nuchal rigidity), or photophobia. See Chapter 13 for further details.
Myocardial Infarction
About a fourth of patients with myocardial infarction will experience nausea and/or vomiting. Check for crushing severe substernal or epigastric pain, with the typical radiation and diaphoresis. See Chapter 9 for more complete workup for myocardial infarction.
Peptic Ulcer Disease
One of the risks with peptic ulcer disease (PUD) is that the erosion may induce an upper GI bleed. If a patient with a history of past or current PUD presents with a recurrence or worsening of symptoms or presents with nausea and or vomiting, the possibility of bleeding from the ulcer needs to be evaluated. Bleeding gastric and duodenal ulcers will produce distinct symptoms. A very large quantity of blood may produce vomitus that consists of bright red blood. This represents a medical emergency and is called hematemesis. If the volume of bleeding is less and it sits in the stomach or small intestine for a period of time before emesis, the vomitus will have the appearance of coffee grounds, which represents partially digested blood. Finally, upper GI bleeding may manifest itself as melena, which are black tarry stools representing significant blood loss from the upper gastrointestinal tract. See Chapters 10 and 25 for further details.
Viral Hepatitis
Early in the course of hepatitis A, nausea and vomiting are common symptoms along with fatigue and flu-like symptoms, including fever. Serum transaminase levels (ALT, AST) are greater than 300 IU/dL. The patient may be jaundiced, have dark urine and elevated bilirubin levels. Elevated IgM anti-HAV antibodies are diagnostic.
Appendicitis
Classical appendicitis presents as RLQ pain. Inflammation may induce the peritoneal reflex, which prevents bowel and bladder emptying. Many cases present with epigastric distress or heartburn and the pain may migrate to the umbilical area before settling in the RLQ. Nausea and vomiting frequently accompany the migration of abdominal discomfort. See Chapter 10 for further details.
Pancreatitis/Cholecystitis
Pancreatitis and cholecystitis can also cause nausea and vomiting. Umbilical pain and tenderness are the hallmark of acute pancreatitis, while right upper quadrant pain is typical in cholecystitis. See Chapter 10 for further details.
Intestinal Obstruction
Intestinal obstruction eventually causes vomiting, often without nausea, along with severe abdominal pain and tenderness. See Chapter 10 for more details.
Pelvic Inflammatory Disease
In females of childbearing age who present with nausea and vomiting, the patient should be queried about a vaginal discharge and recent sexual activity with a new partner, in addition to checking for pregnancy. Most patients with pelvic inflammatory disease (PID) will have a fever plus lower quadrant and suprapubic discomfort or pain in addition to the nausea and vomiting. See Chapter 16 for more details.
Urinary Tract Infection
As above, females of childbearing age presenting with nausea and vomiting should also be asked about dysuria, frequency, fever, urgency and flank pain to rule out acute pyelonephritis (upper urinary tract infection [UTI]). Midstream clean catch urinalysis with large numbers of white cells or bacteria is a quick diagnostic approach. See Chapter 16 for more details.
Uremia
In older patients with long-standing diabetes or prostatic hypertrophy, uremia needs to be ruled out with a urinalysis for protein and/or serum creatinine.
Type 1 Diabetes Mellitus
In patients with Type 1 diabetes mellitus or those with gradual onset of nausea and vomiting, diabetic ketoacidosis needs to be ruled out. Blood tests for plasma glucose and urinalysis for glucose can be quickly used to confirm suspicions of diabetic ketoacidosis.
• KEY REFERENCES
1. Lee NM, Saha S. Nausea and vomiting of pregnancy. Gastroenterol Clin North Am. 2011;40:309-334.
2. Metz A, Hebbard G. Nausea and vomiting in adults. Aust Fam Physician. September 2007;36:688-692.
3. Scorza K, Williams A, Phillips JD, Shaw J. Evaluation of nausea and vomiting. Am Fam Physician. 2007;76:76-84.
4. Getto L, Zeseron E, Breyer M. Vomiting, diarrhea, constipation and gastroenteritis. Emerg Med Clin North Am. 2011;29:211-237.

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


