Nasopharyngeal Angiofibroma
Lester Thompson, MD
Cyril Fisher, MD, DSc, FRCPath
Key Facts
Terminology
Benign, highly cellular, and richly vascularized mesenchymal neoplasm arising in nasopharynx in males
Clinical Issues
Recurrent, spontaneous epistaxis
Nasopharynx is nearly always affected
Patients < 20 years old
Males exclusively
Recurrences in ˜ 20% of patients
Up to 22 cm in size, mean: 4 cm
Image Findings
Anterior bowing of posterior wall of maxillary sinus with posterior displacement of pterygoid plates (Holman-Miller sign)
Angiography identifies feeding vessel(s) and allows for presurgical embolization
Tumor blush is characteristic
Microscopic Pathology
Submucosal proliferation of vascular component within fibrous stroma
Many variably sized disorganized vessels
Fibrous stroma consists of plump spindle, angular, or stellate-shaped cells
Variable amounts of fine and coarse collagen fibers
Elastic tissue is not identified within stroma
Top Differential Diagnoses
Lobular capillary hemangioma
Antrochoanal polyp
Inflammatory polyp
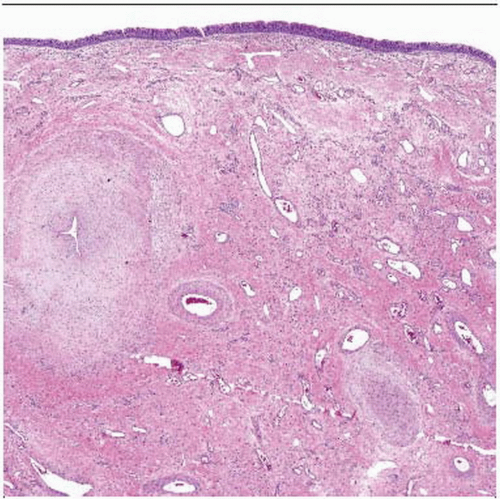 Low magnification shows an intact surface with a wide variety of vessels in a fibrous stroma. Some of the vessels have smooth muscle, and others do not. Patulous and compressed vessels are noted. |
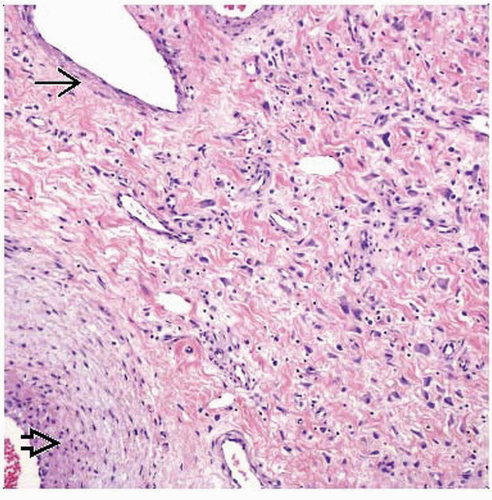 Smooth-muscle-walled vessels  lie close to vessels without smooth muscle lie close to vessels without smooth muscle  . There are also numerous capillaries in the fibrous stroma. The lesion is moderately cellular and lacks atypia. . There are also numerous capillaries in the fibrous stroma. The lesion is moderately cellular and lacks atypia. |
TERMINOLOGY
Abbreviations
Juvenile angiofibroma (JNA)
Angiofibroma (AF)
Synonyms
Angiomyofibroblastoma-like tumor
Angiofibroma
Fibroangioma
Fibroma
Definitions
Benign, highly cellular, and richly vascularized mesenchymal neoplasm arising in nasopharynx in males
ETIOLOGY/PATHOGENESIS
Hormonal
Testosterone-dependent puberty-induced growth can be blocked with estrogen &/or progesterone therapy
Genetic
Reported association with familial adenomatous polyposis
CLINICAL ISSUES
Epidemiology
Incidence
< 1% of all nasopharyngeal tumors
< 0.1% of all head and neck neoplasms
Age
< 20 years old
Adolescents to young men
Peak in 2nd decade of life
Gender
Males exclusively
If diagnosed in female, studies of sex chromosomes required to confirm gender
Ethnicity
Worldwide distribution
Higher frequency in Caucasians
Favors fair-skinned, red-haired individuals
Site
Nasopharynx usually affected
Pterygoid region usually affected
May expand to involve surrounding structures (30% of cases)
Anterior: Nasal cavity and maxillary sinus via roof of nasopharynx
Lateral: Temporal and infratemporal fossae via pterygomaxillary fissure, resulting in cheek or intraoral buccal mass
Posterior: Middle cranial fossa
Superior: Pterygopalatine fossa and orbit via inferior and superior orbital fissures resulting in proptosis
Medial: Contralateral side
Presentation
Nasal obstruction
Recurrent, spontaneous epistaxis
Nasal discharge
Facial deformity (proptosis), exophthalmia, diplopia
Rhinolalia, sinusitis
Otitis media, tinnitus, deafness
Headaches
Rarely, anosmia or pain
Symptoms present for 12-24 months (nonspecific presentation)
Treatment
Options, risks, complications
Benign tumor can show aggressive local growth
Biopsy is contraindicated due to potential exsanguination
Potential for facial deformity if allowed to grow
Surgical approaches
Surgery is treatment of choice
Definitive resection is frequently associated with significant morbidity
Drugs
Preoperative hormone therapy
Not as popular as other modalities
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


