EXAMINATION
Begin examination as patient enters rooms, observing gait and posture. During examination, note ease of movement when patient walks, sits, rises, takes off garments, and responds to directions.
| TECHNIQUE | FINDINGS |
|---|---|
| POSTURE AND GENERAL GUIDELINES | |
| Inspect skeleton and extremities, comparing sides | |
| Inspect anterior, posterior, lateral aspects of posture; ability to stand erect; body parts; extremities. | |
| EXPECTED:Bilateral symmetry of length, circumference, alignment, position and number of skinfolds; symmetric body parts; and aligned extremities. | |
| UNEXPECTED:Gross deformity, lordosis, kyphosis, scoliosis, bony enlargement. | |
| Inspect skin and subcutaneous tissues over muscles, cartilage, bones, joints | |
| UNEXPECTED:Discoloration, swelling, or masses. | |
| Inspect muscles, and compare sides | |
 Size and symmetry Size and symmetry | EXPECTED:Approximately symmetric bilateral muscle size. |
| UNEXPECTED:Gross hypertrophy or atrophy, fasciculations, or spasms. | |
| Palpate all bones, joints, surrounding muscles (palpate inflamed joints last) | |
 Muscle tone Muscle tone | EXPECTED:Firm. |
| UNEXPECTED:Hard or doughy, spasticity. | |
 Characteristics Characteristics | UNEXPECTED:Heat, tenderness, swelling, fluctuation of a joint, synovial thickening, crepitus, resistance to pressure, or discomfort to pressure on bones and joints. |
| Test each major joint and related muscle groups for active and passive range of motion, and compare sides | |
| Ask patient to move each joint through range of motion (see instructions for specific joints and muscles in individual sections that follow), then ask patient to relax as you passively move same joints until end of range is felt. | EXPECTED:Passive range of motion often exceeds active range of motion by 5 degrees. Range of motion with passive and active maneuvers should be equal between contralateral joints. |
| UNEXPECTED:Pain, limitation of motion, spastic movement, joint instability, deformity, contracture, discrepancies greater than 5 degrees between active and passive range of motion. When increase or limitation in range of motion is found, measure angles of greatest flexion and extension with goniometer, as shown in figure below, and compare with values as described for specific joints in individual extremities. | |
| Test major muscle groups for strength, and compare contralateral sides | |
| For each muscle group, ask patient to contract a muscle by flexing or extending a joint and to resist as you apply opposing force. Compare bilaterally. | EXPECTED:Bilaterally symmetric strength with full resistance to opposition. |
| UNEXPECTED:Inability to produce full resistance. Grade muscular strength according to table below. | |


| Muscle Function Level | Grade |
|---|---|
| No evidence of contractility | 0 |
| Slight contractility, no movement | 1 |
| Full range of motion, gravity eliminated* | 2 |
| Full range of motion against gravity | 3 |
| Full range of motion against gravity, some resistance | 4 |
| Full range of motion against gravity, full resistance | 5 |
From Jacobson, 1998.
| TECHNIQUE | FINDINGS |
|---|---|
| HANDS AND WRISTS | |
| Inspect dorsum and palm of each hand | |
 Characteristics and contour Characteristics and contour | EXPECTED:Palmar and phalangeal creases, palmar surfaces with central depression with prominent, rounded mound on thumb side (thenar eminence) and less prominent hypothenar eminence on little-finger side. |
 Position Position | EXPECTED:Fingers able to fully extend and aligned with forearm when in close approximation to each other. |
| UNEXPECTED:Deviation of fingers to ulnar side or inability to fully extend fingers; swan neck or boutonnière deformities. | |
 Shape Shape | EXPECTED:Lateral finger surfaces gradually tapered from proximal to distal aspects. |
| UNEXPECTED:Spindle-shaped fingers, bony overgrowths at phalangeal joints. | |
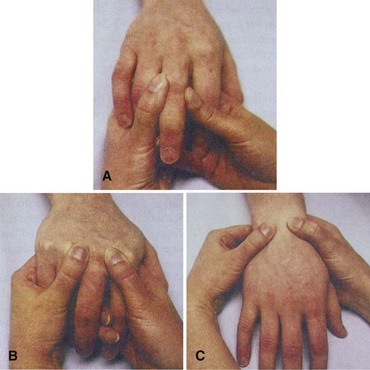
| Palpate each joint in hand and wrist | |
| Palpate interphalangeal joints with thumb and index finger, as shown in the figure on p. 220, A; metacarpophalangeal joints with both thumbs, as shown in the figure on p. 220, B; and wrist and radiocarpal groove with thumbs on dorsal surface and fingers on palmar aspect of wrist, as shown in the figure on p. 220, C. | EXPECTED:Joint surfaces smooth. |
| UNEXPECTED:Nodules, swelling, bogginess, tenderness, or ganglion. | |
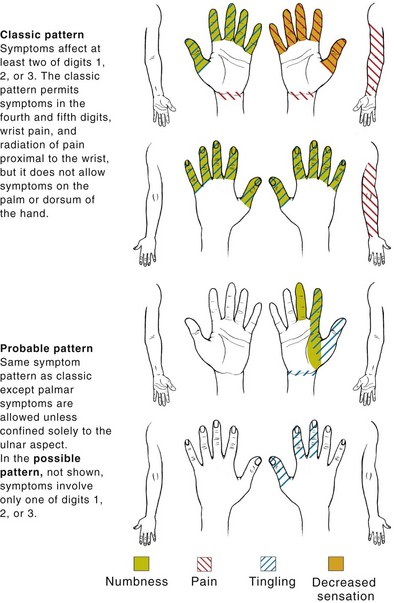
| Assess integrity of median nerve | |
| UNEXPECTED:Tingling sensation radiating from wrist to hand along pathway of median nerve. | |
| EXPECTED:Full resistance to pressure. | |
| UNEXPECTED:Inability to produce full resistance. | |
| UNEXPECTED:Numbness, paresthesia in distribution of median nerve. | |
| UNEXPECTED:Pain, numbness, tingling in pattern shown in figure on below. | |
| Test range of motion | |
| Ask patient to perform the following movements: | |
| EXPECTED:90-degree metacarpophalangeal flexion and as much as 30-degree hyperextension. | |
| EXPECTED:Able to perform all movements. | |
| EXPECTED:Both movements possible. | |
| EXPECTED:90-degree flexion and 70-degree hyperextension. | |
| EXPECTED:20-degree radial motion and 55-degree ulnar motion. | |
| Test muscle strength | |
| Ask patient to perform the following movements: | |
| EXPECTED:Bilaterally symmetric with full resistance to opposition. | |
| UNEXPECTED:Inability to produce full resistance. | |
| EXPECTED:Firm, sustained grip. | |
| UNEXPECTED:Weakness or pain. | |
| ELBOWS | |
| Inspect elbows in flexed and extended positions | |
 Contour Contour | UNEXPECTED:Subcutaneous nodules along pressure points of extensor surface of ulna. |
| EXPECTED:Usually 5 to 15 degrees laterally. | |
| UNEXPECTED:Lateral angle exceeding 15 degrees (cubitus valgus) or a medial carrying angle (cubitus varus). | |
| Palpate extensor surface of ulna, olecranon process, medial and lateral epicondyles of humerus, groove on each side of olecranon process | |
| Palpate with patient’s elbow flexed at 70 degrees. | UNEXPECTED:Boggy, soft, tenderness at lateral epicondyle or along grooves of olecranon process and epicondyles. |
| Test range of motion | |
| Ask patient to perform the following movements: | |
| EXPECTED:160-degree flexion from full extension at 0 degrees. | |
| EXPECTED:90-degree pronation and 90-degree supination. | |
| UNEXPECTED:Increased pain with pronation and supination of elbow. | |
| Test muscle strength | |
| Ask patient to maintain flexion and extension, as well as pronation and supination, while you apply opposing force. | EXPECTED:Bilaterally symmetric with full resistance to opposition. |
| UNEXPECTED:Inability to produce full resistance. | |
| SHOULDERS | |
| Inspect shoulders, shoulder girdle, clavicles and scapulae, area muscles | |
 Size and contour Size and contour | EXPECTED:All shoulder structures symmetric in size and contour. |
| UNEXPECTED:Asymmetry, hollows in rounding contour, or winged scapula. | |
| Palpate sternoclavicular and acromioclavicular joints, clavicle, scapulae, coracoid process, greater trochanter of humerus, biceps groove, area muscles | |
Palpate the biceps groove by rotating the arm and forearm externally. Follow the biceps muscle and tendon along the anterior aspect of the humerus into the biceps groove. | |
| Test range of motion | |
| Ask patient to perform the following movements: | |
 Shoulder shrug Shoulder shrug | EXPECTED:Symmetric rising. |
| EXPECTED:180-degree forward flexion. | |
| EXPECTED:50-degree hyperextension. | |
| EXPECTED:180-degree abduction. | |
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

| |