Chapter 19 Musculoskeletal System
Bisphosphonates (BPs)




MOA (Mechanism of Action)
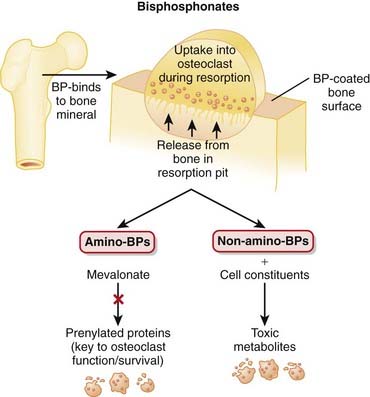
 The structural integrity of bone is determined to a large extent by the balance between the activity of osteoclasts, which break down bone (resorptive), and the activity of osteoblasts, which build bone.
The structural integrity of bone is determined to a large extent by the balance between the activity of osteoclasts, which break down bone (resorptive), and the activity of osteoblasts, which build bone. Bisphosphonates (BPs) inhibit osteoclast activity through a variety of mechanisms, some better understood than others (Figure 19-1).
Bisphosphonates (BPs) inhibit osteoclast activity through a variety of mechanisms, some better understood than others (Figure 19-1).




Pharmacokinetics
 BPs have very low oral bioavailability (<10%), and their absorption is further reduced by food and by divalent cations such as calcium. It is therefore recommended that BPs be taken on an empty stomach, with plain water.
BPs have very low oral bioavailability (<10%), and their absorption is further reduced by food and by divalent cations such as calcium. It is therefore recommended that BPs be taken on an empty stomach, with plain water.









Contraindications
 Hypocalcemia: BPs have exhibited decreases in serum calcium, so it is recommended that any deficiencies in calcium be addressed before initiation of therapy.
Hypocalcemia: BPs have exhibited decreases in serum calcium, so it is recommended that any deficiencies in calcium be addressed before initiation of therapy.
Side Effects
All

Serious
 Esophagitis or esophageal erosion is more commonly seen with the aminobisphosphonates. It may result from a direct irritant effect from tablets lodged in the esophagus or from reflux of gastric acid including the acidic form of the BP. Patients are advised to avoid reclining for at least 30 minutes after taking a BP, reducing the chance of tablet staying in the esophagus or reflux.
Esophagitis or esophageal erosion is more commonly seen with the aminobisphosphonates. It may result from a direct irritant effect from tablets lodged in the esophagus or from reflux of gastric acid including the acidic form of the BP. Patients are advised to avoid reclining for at least 30 minutes after taking a BP, reducing the chance of tablet staying in the esophagus or reflux.

Important Notes
 The non-aminobisphosphonates were the original members of this drug class, whereas the aminobisphosphonates are newer, more potent agents.
The non-aminobisphosphonates were the original members of this drug class, whereas the aminobisphosphonates are newer, more potent agents.




Evidence
Risedronate versus Placebo or Calcium and Vitamin D or Both in Postmenopausal Osteoporosis
 A 2008 Cochrane review (7 trials, N = 14,049 females) found no statistically significant effects for risedronate with respect to primary prevention of vertebral and nonvertebral fractures. For secondary prevention, risedronate demonstrated statistically significant relative risk reductions (RRRs) of vertebral fractures (39%), nonvertebral fractures (20%), and hip fractures (26%). The corresponding absolute risk reductions were small: 5%, 2%, and 1%, respectively. No statistically significant differences were found for adverse events.
A 2008 Cochrane review (7 trials, N = 14,049 females) found no statistically significant effects for risedronate with respect to primary prevention of vertebral and nonvertebral fractures. For secondary prevention, risedronate demonstrated statistically significant relative risk reductions (RRRs) of vertebral fractures (39%), nonvertebral fractures (20%), and hip fractures (26%). The corresponding absolute risk reductions were small: 5%, 2%, and 1%, respectively. No statistically significant differences were found for adverse events.Etidronate versus Placebo and/or Calcium and Vitamin D in Postmenopausal Osteoporosis
 A 2008 Cochrane review (11 trials, N = 1248 females) found no statistically significant effects of etidronate with respect to primary prevention of any fractures. A statistically significant RRR of 47% was found for secondary prevention of vertebral fractures but not for nonvertebral, hip, or wrist fractures. No statistically significant differences were found for adverse events.
A 2008 Cochrane review (11 trials, N = 1248 females) found no statistically significant effects of etidronate with respect to primary prevention of any fractures. A statistically significant RRR of 47% was found for secondary prevention of vertebral fractures but not for nonvertebral, hip, or wrist fractures. No statistically significant differences were found for adverse events.BPs versus Placebo or No Treatment in Myeloma
 A 2002 Cochrane review (11 trials, N = 2183 patients) found that BPs prevented pathologic vertebral fractures (number needed to treat [NNT] = 10) and relieved pain (NNT = 11). BPs did not affect mortality, nonvertebral fractures, or hypercalcemia. No significant adverse events were associated with the BPs.
A 2002 Cochrane review (11 trials, N = 2183 patients) found that BPs prevented pathologic vertebral fractures (number needed to treat [NNT] = 10) and relieved pain (NNT = 11). BPs did not affect mortality, nonvertebral fractures, or hypercalcemia. No significant adverse events were associated with the BPs.




Vitamin D Replacement


MOA (Mechanism of Action)

 Vitamin D is an important regulator of calcium and phosphate homeostasis and bone metabolism. It works in conjunction with PTH. The overall effect of vitamin D is to increase serum calcium concentrations. These effects are mediated via the following:
Vitamin D is an important regulator of calcium and phosphate homeostasis and bone metabolism. It works in conjunction with PTH. The overall effect of vitamin D is to increase serum calcium concentrations. These effects are mediated via the following:















Important Notes
 Vitamin D is synthesized in the skin, liver, and kidney. Vitamin D supplementation is therefore frequently required in patients with renal failure.
Vitamin D is synthesized in the skin, liver, and kidney. Vitamin D supplementation is therefore frequently required in patients with renal failure.


Advanced
 Vitamin D supplements are sometimes used in the treatment of psoriasis, a common skin condition involving rapid turnover and inflammation of the skin. The evidence for this use, however, is not strongly conclusive.
Vitamin D supplements are sometimes used in the treatment of psoriasis, a common skin condition involving rapid turnover and inflammation of the skin. The evidence for this use, however, is not strongly conclusive. The various forms of vitamin D are referred to by several different names, summarized in Table 19-1.
The various forms of vitamin D are referred to by several different names, summarized in Table 19-1.TABLE 19-1 Various Forms of Vitamin D
| Common Name | Drug Name | Abbreviation |
|---|---|---|
| Vitamin D2 | Ergocalciferol | D2 |
| 1-Hydroxyvitamin D2 | Doxercalciferol | 1(OH)D2 |
| Vitamin D3 | Cholecalciferol | D3 |
| 25-Hydroxyvitamin D3 | Calcifediol | 25(OH)D3 |
| 1,25-Dihydroxyvitamin D3 | Calcitriol | 1,25(OH)2D3 |
| 24,25-Dihydroxyvitamin D3 | Secalcifediol | 24,25(OH)2D3 |
Evidence

Vitamin D Plus Calcium and Bone Fractures in the Elderly
 The same meta-analysis in 2008 showed that vitamin D plus calcium supplements do reduce hip fractures in the elderly (8 trials, N = 46,658 participants, relative risk [RR] 0.84). Hypercalcemia is significantly more common in people receiving vitamin D or an analogue, with or without calcium (18 trials, N = 11,346 participants, RR 2.35). There is a significant but modest increase in gastrointestinal symptoms (RR 1.04) and a small but significant increase in renal disease (RR 1.16).
The same meta-analysis in 2008 showed that vitamin D plus calcium supplements do reduce hip fractures in the elderly (8 trials, N = 46,658 participants, relative risk [RR] 0.84). Hypercalcemia is significantly more common in people receiving vitamin D or an analogue, with or without calcium (18 trials, N = 11,346 participants, RR 2.35). There is a significant but modest increase in gastrointestinal symptoms (RR 1.04) and a small but significant increase in renal disease (RR 1.16).FYI
 The concept that vitamin D comes from the sun is inaccurate; the inert precursor (7-dehydrocholesterol) is present in the skin, and exposure to ultraviolet light converts it to cholecalciferol, which is then isomerized to vitamin D3. Reduced exposure to sunlight is one cause of vitamin D deficiency.
The concept that vitamin D comes from the sun is inaccurate; the inert precursor (7-dehydrocholesterol) is present in the skin, and exposure to ultraviolet light converts it to cholecalciferol, which is then isomerized to vitamin D3. Reduced exposure to sunlight is one cause of vitamin D deficiency.

Parathyroid Hormone

MOA (Mechanism of Action)
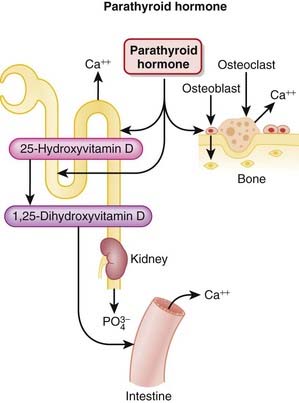
 PTH is released from the parathyroid gland. It regulates calcium and phosphate flux across cell membranes in bone and kidney. The key effects of PTH are as follows:
PTH is released from the parathyroid gland. It regulates calcium and phosphate flux across cell membranes in bone and kidney. The key effects of PTH are as follows:



 The stimulation of osteoclasts increases bone remodeling. PTH increases both bone resorption and formation; however, the net effect of excess PTH is to increase bone resorption (Figure 19-3).
The stimulation of osteoclasts increases bone remodeling. PTH increases both bone resorption and formation; however, the net effect of excess PTH is to increase bone resorption (Figure 19-3).