Figure 6-1. Mood episodes. Bipolar disorder is generally characterized by four types of illness episodes: manic, major depressive, hypomanic, and mixed. A patient may have any combination of these episodes over the course of illness; subsyndromal manic or depressive episodes also occur during the course of illness, in which case there are not enough symptoms or the symptoms are not severe enough to meet the diagnostic criteria for one of these episodes. Thus the presentation of mood disorders can vary widely.
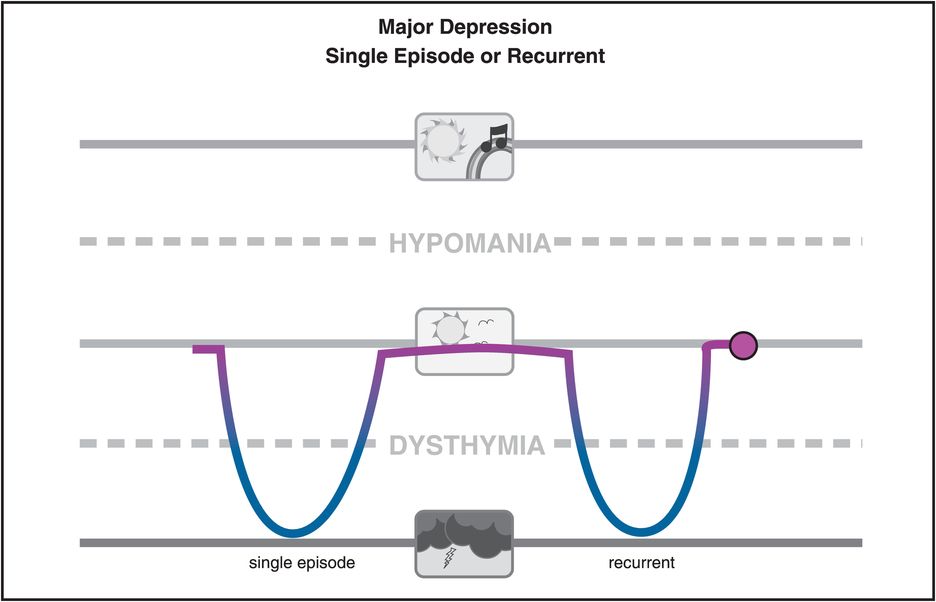
Figure 6-2. Major depression. Major depression is the most common mood disorder and is defined by the occurrence of at least a single major depressive episode, although most patients will experience recurrent episodes.
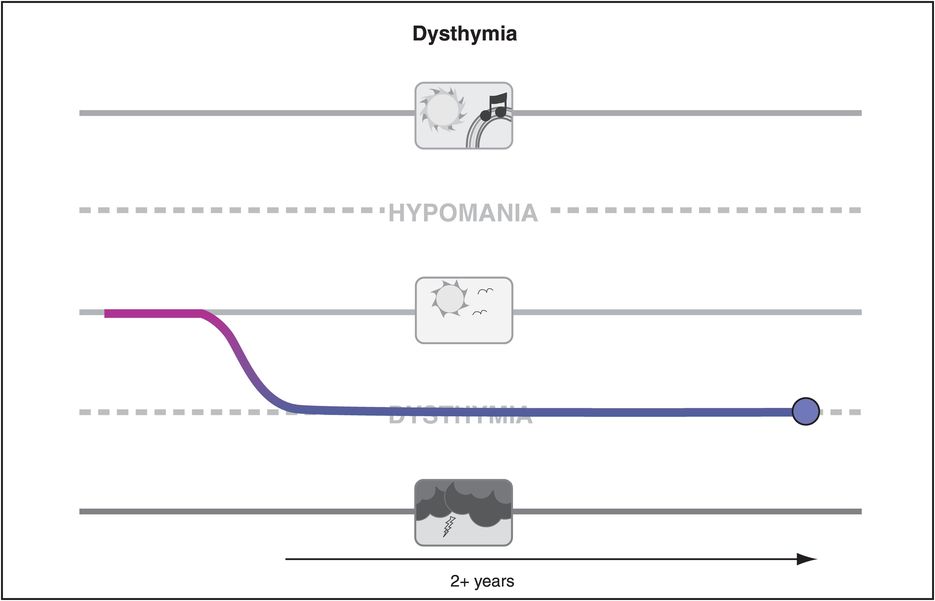
Figure 6-3. Dysthymia. Dysthymia is a less severe form of depression than major depression, but long-lasting (over 2 years in duration) and often unremitting.
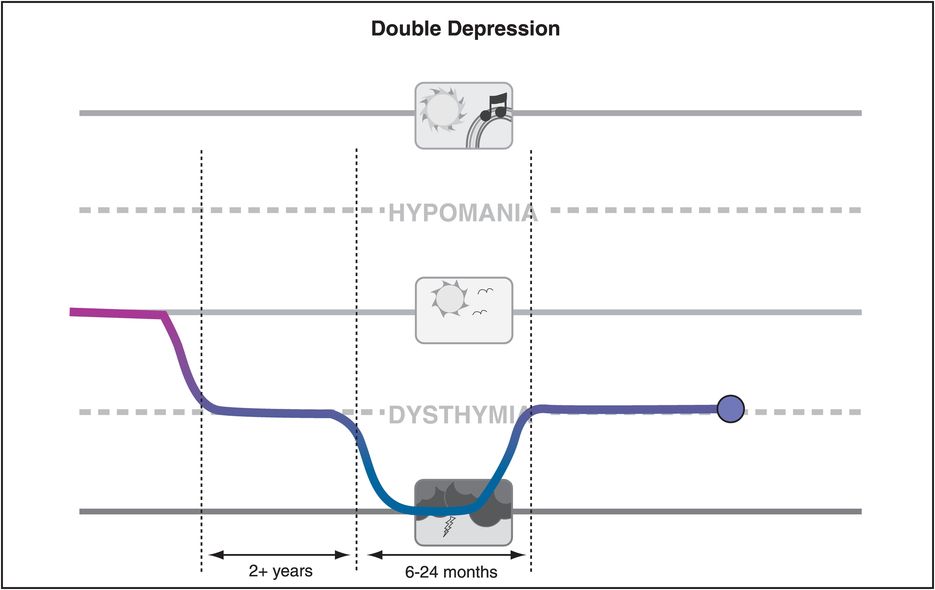
Figure 6-4. Double depression. Patients with unremitting dysthymia who also experience the superimposition of one or more major depressive episodes are described as having double depression. This is also a form of recurrent major depressive episodes with poor inter-episode recovery.
Patients with bipolar I disorder have full-blown manic episodes or mixed episodes of mania plus depression, often followed by a depressive episode (Figure 6-5). When mania recurs at least four times a year, it is called rapid cycling (Figure 6-6A). Patients with bipolar I disorder can also have rapid switches from mania to depression and back (Figure 6-6B). By definition, this occurs at least four times a year, but can occur much more frequently than that.
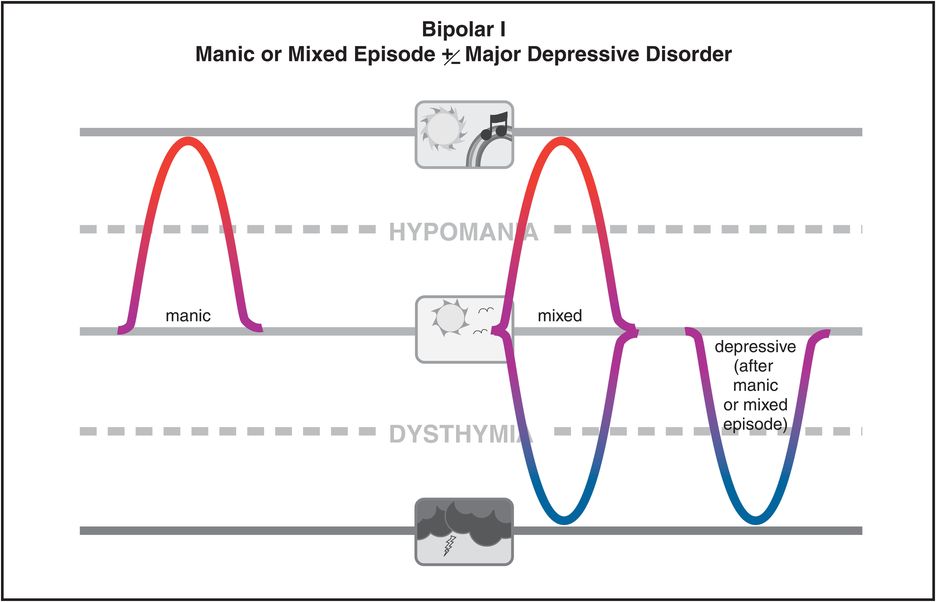
Figure 6-5. Bipolar I disorder. Bipolar I disorder is defined as the occurrence of at least one manic or mixed (full mania and full depression simultaneously) episode. Patients with bipolar I disorder typically experience major depressive episodes as well, although this is not necessary for the bipolar I diagnosis.
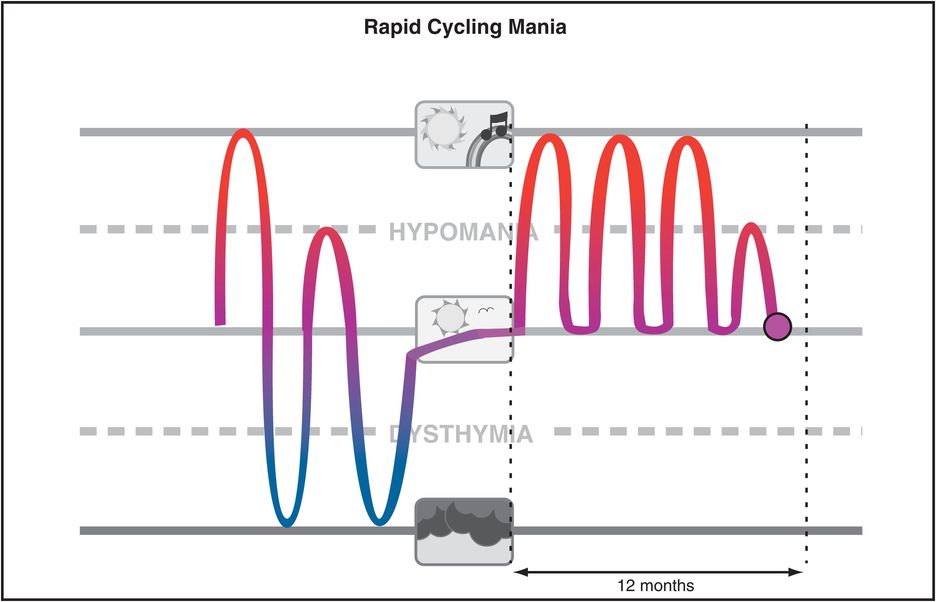
A. Rapid cycling mania. The course of bipolar disorder can be rapid cycling, which means that at least four episodes occur within a 1-year period. This can manifest itself as four distinct manic episodes, as shown here. Many patients with this form of mood disorder experience switches much more frequently than four times a year.
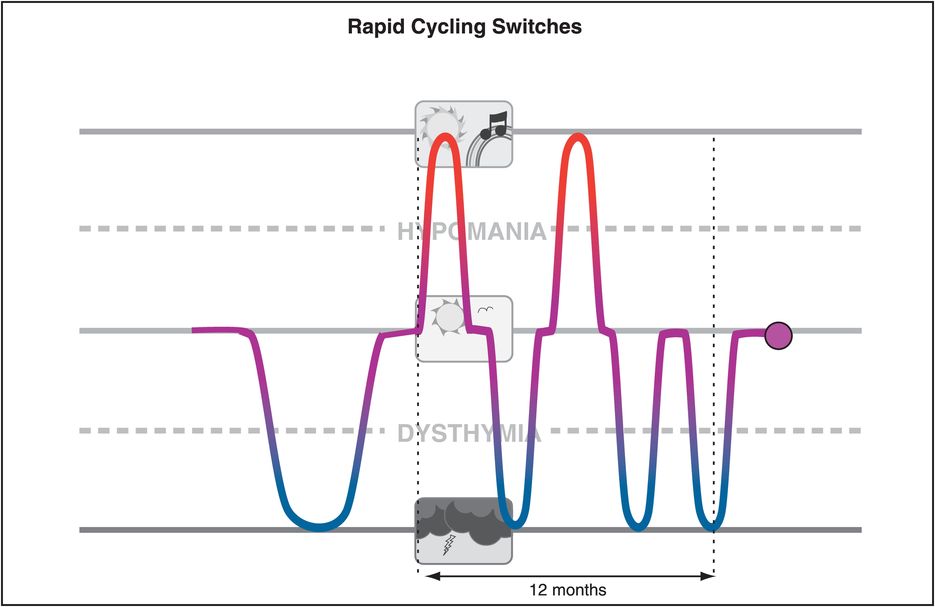
B. Rapid cycling switches. A rapid cycling course (at least four distinct mood episodes within 1 year) can also manifest as rapid switches between manic and depressive episodes.
Bipolar II disorder is characterized by at least one hypomanic episode that follows a depressive episode (Figure 6-7). Cyclothymic disorder is characterized by mood swings that are not as severe as full mania and full depression, but still wax and wane above and below the boundaries of normal mood (Figure 6-8). There may be lesser degrees of variation from normal mood that are stable and persistent, including both depressive temperament (below normal mood but not a mood disorder) and hyperthymic temperament (above normal mood but also not a mood disorder) (Figure 6-9). Temperaments are personality styles of responding to environmental stimuli that can be heritable patterns present early in life and persisting throughout a lifetime; temperaments include such independent personality dimensions as novelty seeking, harm avoidance, and conscientiousness. Some patients may have mood-related temperaments, and these may render them vulnerable to mood disorders, especially bipolar spectrum disorders, later in life.
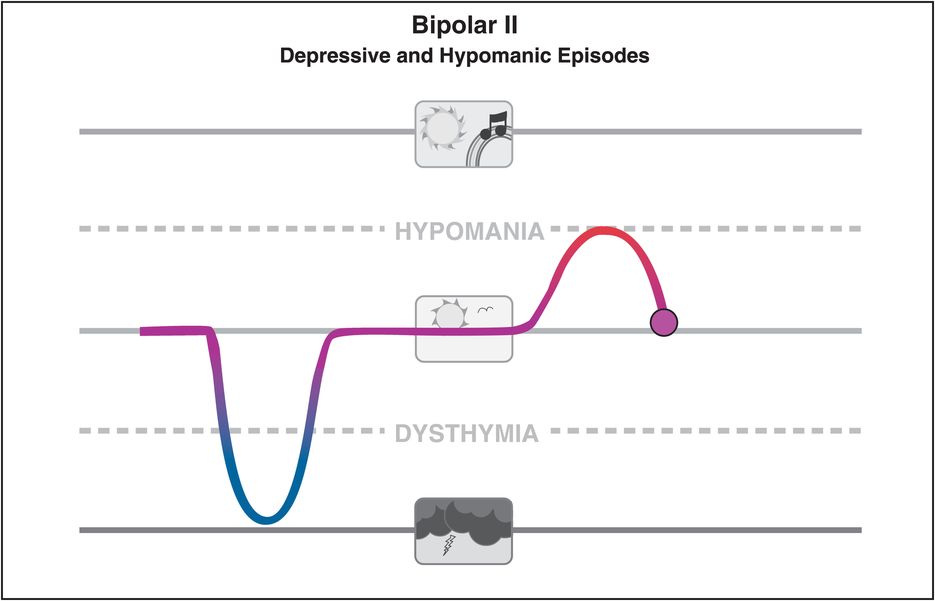
Figure 6-7. Bipolar II disorder. Bipolar II disorder is defined as an illness course consisting of one or more major depressive episodes and at least one hypomanic episode.
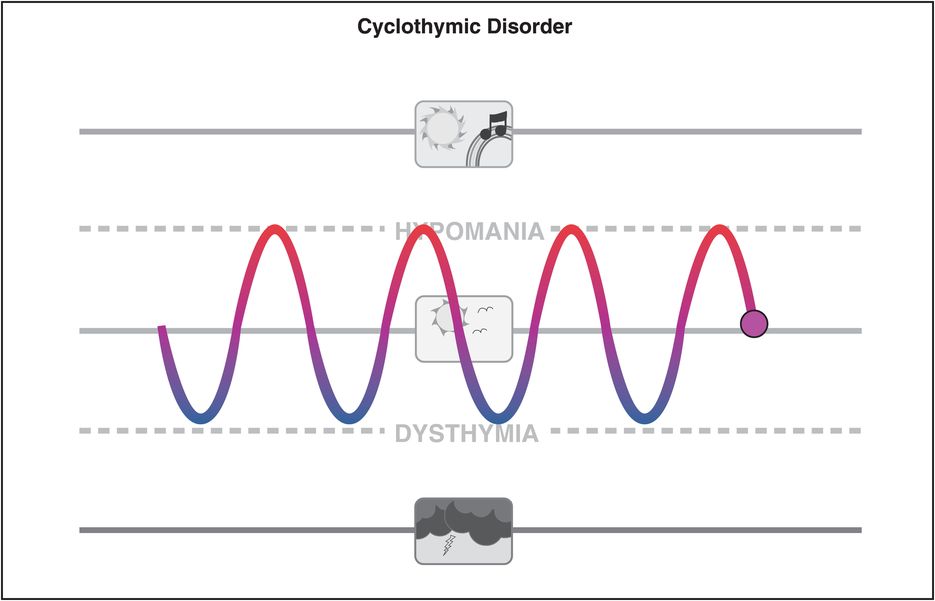
Figure 6-8. Cyclothymic disorder. Cyclothymic disorder is characterized by mood swings between hypomania and dysthymia but without any full manic or major depressive episodes.
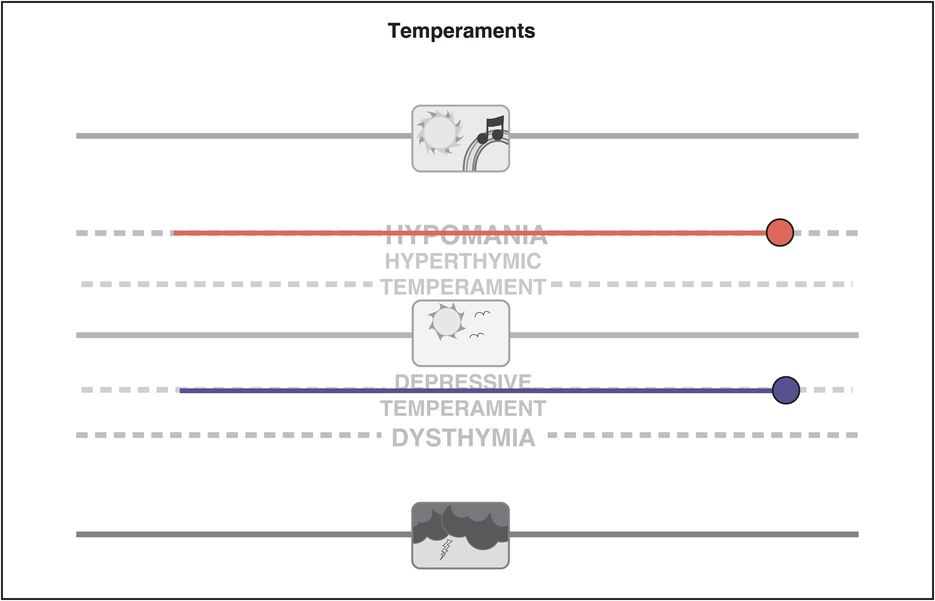
Figure 6-9. Temperaments. Not all mood variations are pathological. Individuals with depressive temperament may be consistently sad or apathetic but do not meet the criteria for dysthymia and do not necessarily experience any functional impairment. However, individuals with depressive temperament may be at greater risk for the development of a mood disorder later in life. Hyperthymic temperament, in which mood is above normal but not pathological, includes stable characteristics such as extroversion, optimism, exuberance, impulsiveness, overconfidence, grandiosity, and lack of inhibition. Individuals with hyperthymic temperament may be at greater risk for the development of a mood disorder later in life.
The bipolar spectrum
From a strict diagnostic point of view, our discussion of mood disorders could now be mostly complete. However, there is the growing recognition that many patients seen in clinical practice have a mood disorder not well described by the above categories. Formally, they would be called “not otherwise specified” or “NOS,” but this creates a huge single category for many patients that belies the richness and complexity of their symptoms. Increasingly, such patients are seen as belonging in general to the “bipolar spectrum” (Figure 6-10), and in particular to one of several additional descriptive categories that have been proposed by experts such as Hagop Akiskal (Figures 6-10 through 6-20).
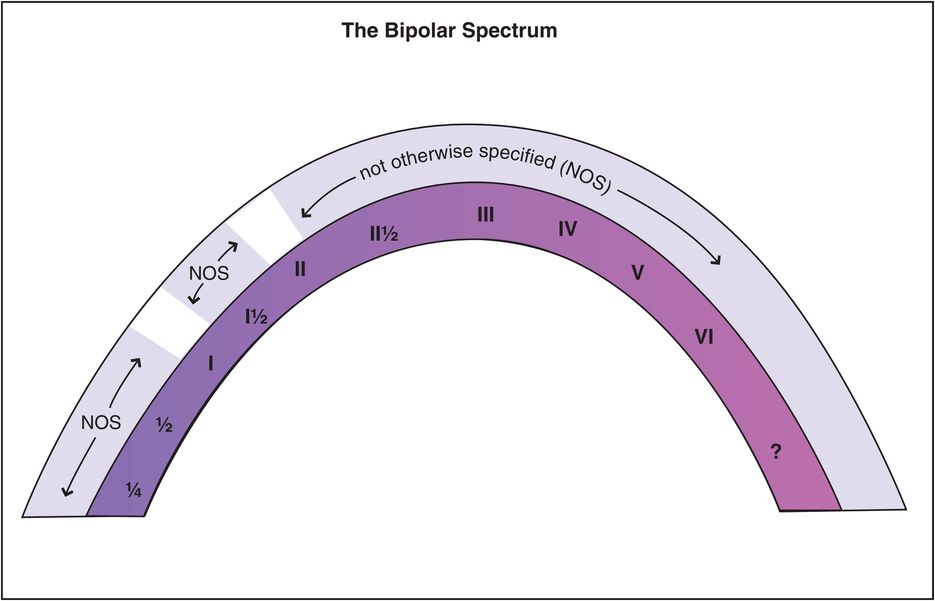
Figure 6-10. Bipolar spectrum. There is a huge variation in the presentation of patients with bipolar disorder. Historically, bipolar disorder has been categorized as I, II, or not otherwise specified (NOS). It may be more useful, instead, to think of these patients as belonging to a bipolar spectrum and to identify subcategories of presentations, as has been done by Akiskal and other experts and as illustrated in the next several figures.
Bipolar ¼ (0.25)
One mood disorder often considered to be “not quite bipolar” and sometimes called bipolar ¼ (or 0.25) designates an unstable form of unipolar depression that responds sometimes rapidly but in an unsustained manner to antidepressants, the latter sometimes called antidepressant “poop-out” (Figure 6-11). These patients have unstable mood but not a formal bipolar disorder, yet can benefit from mood-stabilizing treatments added to robust antidepressant treatments.
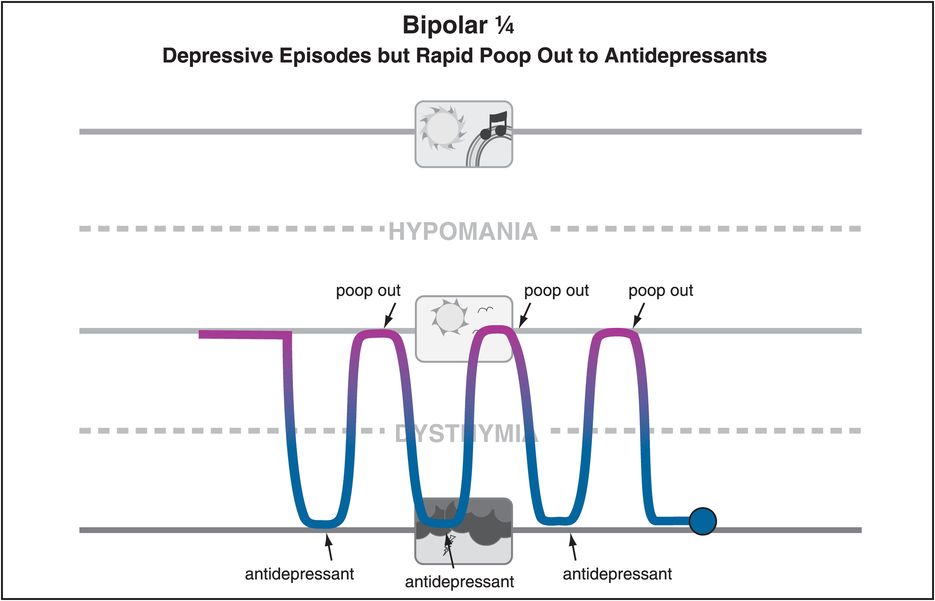
Figure 6-11. Bipolar ¼. Some patients may present only with depressive symptoms yet exhibit rapid but unsustained response to antidepressant treatment (sometimes called rapid “poop out”). Although such patients may have no spontaneous mood symptoms above normal, they potentially could benefit from mood-stabilizing treatment. This presentation may be termed bipolar ¼ (or bipolar 0.25).
Bipolar ½ (0.5) and schizoaffective disorder
Another type of mood disorder is called different things by different experts, from bipolar ½ (or 0.5) to “schizobipolar disorder” to “schizoaffective disorder” (Figure 6-12). For over a century, experts have debated whether psychotic disorders are dichotomous from mood disorders (Figure 6-13A) or are part of a continuous disease spectrum from psychosis to mood (Figure 6-13B).
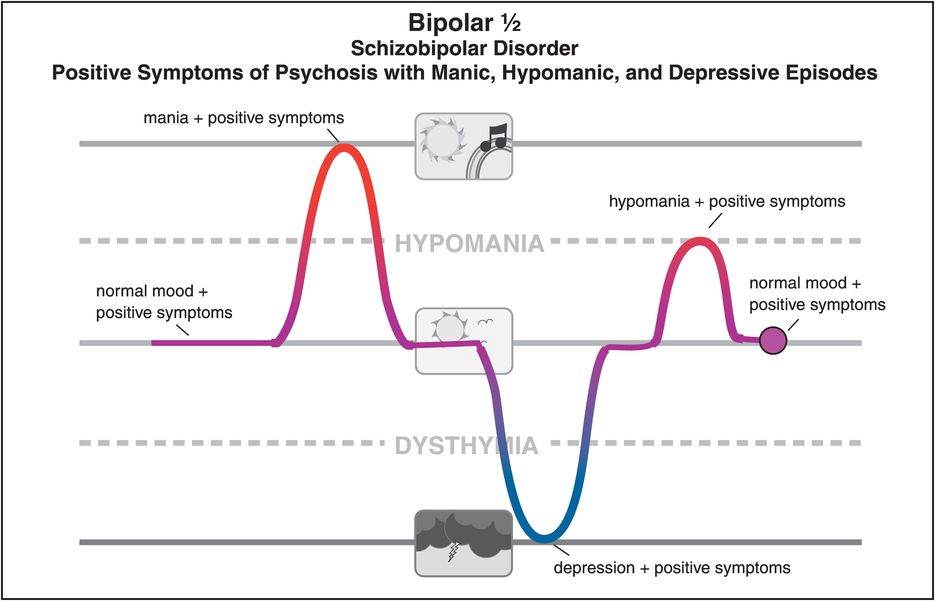
Figure 6-12. Bipolar ½. Bipolar ½ (0.5) has been described as schizobipolar disorder, which combines positive symptoms of psychosis with manic, hypomanic, and depressive episodes.
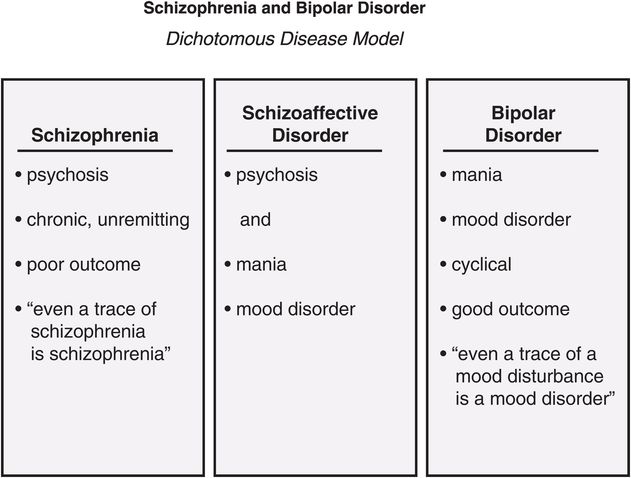
A. Schizophrenia and bipolar disorder: dichotomous disease model. Schizophrenia and bipolar disorder have been conceptualized both as dichotomous disorders and as belonging to a continuum. In the dichotomous disease model, schizophrenia consists of chronic, unremitting psychosis, with poor outcomes expected. Bipolar disorder consists of cyclical manic and other mood episodes and has better expected outcomes than schizophrenia. A third distinct disorder is schizoaffective disorder, characterized by psychosis and mania as well as other mood symptoms.
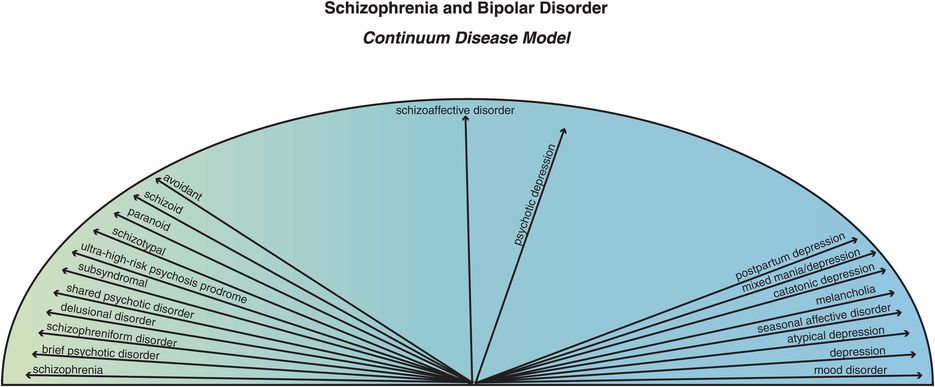
B. Schizophrenia and bipolar disorder: continuum disease model. Schizophrenia and bipolar disorder have been conceptualized both as dichotomous disorders and as belonging to a continuum. In the continuum disease model, schizophrenia and mood disorders fall along a continuum in which psychosis, delusions, and paranoid avoidant behavior are on one extreme and depression and other mood symptoms are on the other extreme. Falling in the middle are psychotic depression and schizoaffective disorder.
The dichotomous disease model is in the tradition of Kraepelin and proposes that schizophrenia is a chronic unremitting illness with poor outcome and decline in function whereas bipolar disorder is a cyclical illness with a better outcome and good restoration of function between episodes. However, there is great debate as to how to define the borders between these two illnesses. One notion is that cases with overlapping symptoms and intermediate disease courses can be seen as a third illness, schizoaffective disorder. Today, many define this border with the idea that “even a trace of schizophrenia is schizophrenia.” From this “schizophrenia-centered perspective,” many overlapping cases of psychotic mania and psychotic depression might be considered either to be forms of schizophrenia, or to be schizoaffective disorder as a form of schizophrenia with affective symptoms. A competing point of view within the dichotomous model is that “even a trace of mood disturbance is a mood disorder.” From this “mood-centered perspective,” many overlapping cases of psychotic mania and psychotic depression might be considered either to be forms of a mood/bipolar disorder or to be schizoaffective disorder as a form of mood/bipolar disorder with psychotic symptoms. Where patients have a mixture of mood symptoms and psychosis, it can obviously be very difficult to tell whether they have a psychotic disorder such as schizophrenia, a mood disorder such as bipolar disorder, or a third condition, schizoaffective disorder. Some even want to eliminate the diagnosis of schizoaffective disorder entirely.
Proponents of the dichotomous model point out that treatments for schizophrenia differ from those for bipolar disorder, since lithium is rarely helpful in schizophrenia, and anticonvulsant mood stabilizers have limited efficacy for psychotic symptoms in schizophrenia, and perhaps only as augmenting agents. Treatments for schizoaffective disorder can include both treatments for schizophrenia and treatments for bipolar disorder. The current debate within the dichotomous model is: If you have bipolar disorder, do you have a good outcome? – but if you have schizophrenia, do you have a poor outcome? – and what genetic and biological markers rather than clinical symptoms can distinguish one dichotomous entity from the other?
The continuum disease model proposes that psychotic and mood disorders are both manifestations of one complex set of disorders that is expressed across a spectrum, at one end schizophrenia (plus schizophreniform disorder, brief psychotic disorder, delusional disorder, shared psychotic disorder, subsyndromal/ultra-high-risk psychosis prodrome, schizotypal, paranoid, schizoid, and even avoidant personality disorders), and at the other end bipolar/mood disorders (mania, depression, mixed states, melancholic depression, atypical depression, catatonic depression, postpartum depression, psychotic depression, seasonal affective disorder), with schizoaffective disorder in the middle, combining features of positive symptoms of psychosis with manic, hypomanic, or depressive episodes (Figure 6-13B).
Modern genomics suggests that the spectrum is not a single disease, but a complex of hundreds if not thousands of different diseases, with overlapping genetic, epigenetic, and biomarkers as well as overlapping clinical symptoms and functional outcomes. Proponents of the continuum model point out that treatments for schizophrenia overlap greatly now with those for bipolar disorder, since second-generation atypical antipsychotics are effective in the positive symptoms of schizophrenia and in psychotic mania and psychotic depression, and are also effective in nonpsychotic mania and in bipolar depression and unipolar depression. These same second-generation atypical antipsychotics are effective for the spectrum of symptoms in schizoaffective disorder. From the continuum disease perspective, failure to give mood-stabilizing medications may lead to suboptimal symptom relief in patients with psychosis, even those whose prominent or eye-catching psychotic symptoms mask or distract clinicians from seeing underlying and perhaps more subtle mood symptoms. In the continuum disease model, schizophrenia can be seen as the extreme end of a spectrum of severity of mood disorders and not a disease unrelated to a mood disorder. Schizophrenia can therefore share with schizoaffective disorder severe psychotic symptoms that obscure mood symptoms, a chronic course that eliminates cycling, resistance to antipsychotic treatments, and prominent negative symptoms, yet be just a severe form of the same illness. In the continuum disease model, schizoaffective disorder would be a milder form of the illness with less severe psychotic features and more severe mood features.
The debate rages on . . .
Bipolar I½ (1.5)
Although patients with protracted or recurrent hypomania without depression are not formally diagnosed as bipolar II disorder, they are definitely part of the bipolar spectrum, and may benefit from mood stabilizers that have been studied mostly in bipolar I disorder (Figure 6-14). Eventually, such patients will often develop a major depressive episode and their diagnosis will then change to bipolar II disorder, but in the meantime they can be treated for hypomania while being vigilant to the future onset of a major depressive episode.
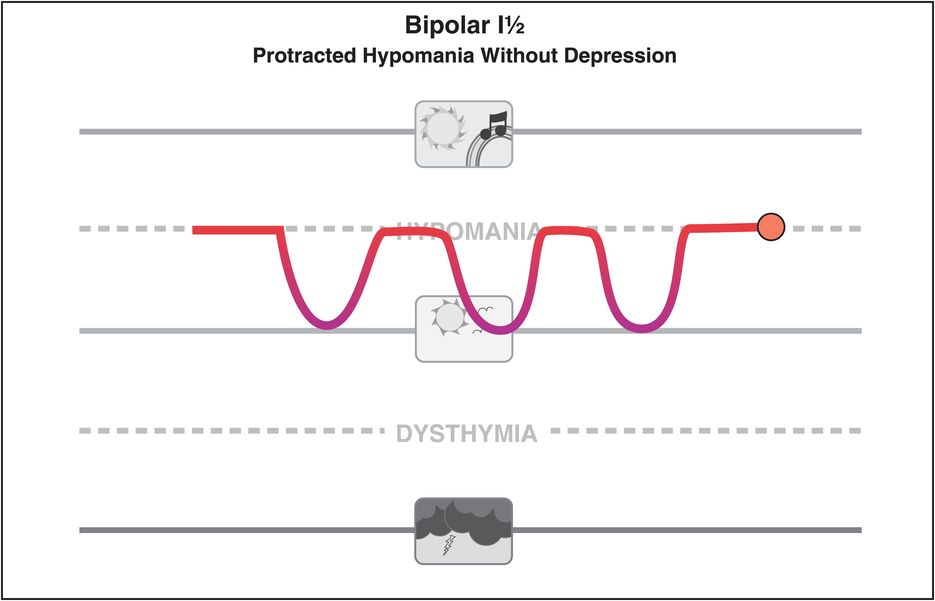
Figure 6-14. Bipolar I½. A formal diagnosis of bipolar II disorder requires the occurrence of not only hypomanic episodes but also depressive episodes. However, some patients may experience recurrent hypomania without having experienced a depressive episode – a presentation that may be termed bipolar I½. These patients may be at risk of eventually developing a depressive episode and are candidates for mood-stabilizing treatment, although no treatment is formally approved for this condition.
Bipolar II½ (2.5)
Bipolar II½ is the designation for cyclothymic patients who develop major depressive episodes (Figure 6-15). Many patients with cyclothymia are just considered “moody” and do not consult professionals until experiencing full depressive episodes. It is important to recognize patients in this part of the bipolar spectrum, because treatment of their major depressive episodes with antidepressant monotherapy may actually cause increased mood cycling or even induction of a full manic episode, just as can happen in patients with bipolar I or II depressive episodes.
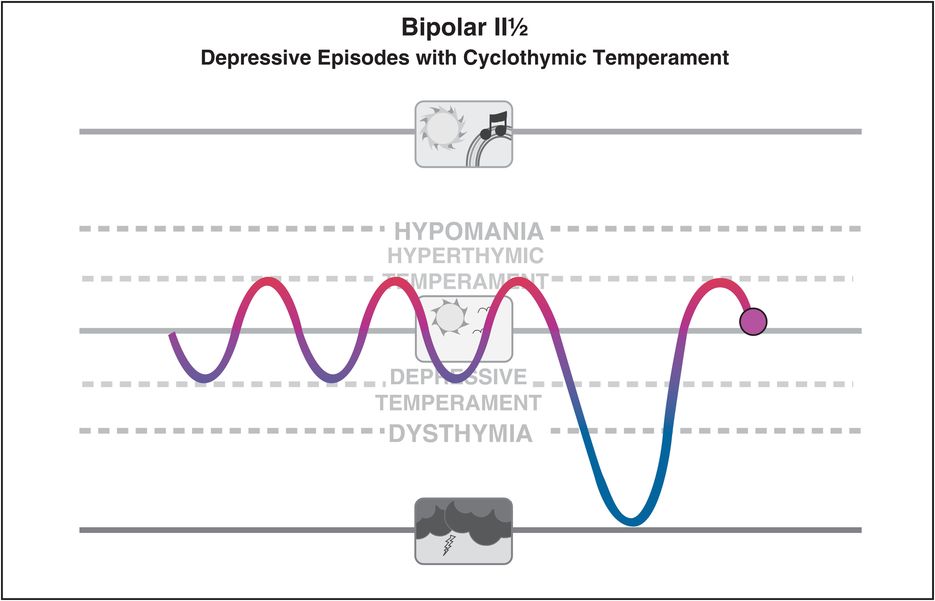
Figure 6-15. Bipolar II½. Patients may present with a major depressive episode in the context of cyclothymic temperament, which is characterized by oscillations between hyperthymic or hypomanic states (above normal) and depressive or dysthymic states (below normal) upon which a major depressive episode intrudes (bipolar II½). Individuals with cyclothymic temperament who are treated for the major depressive episodes may be at increased risk for antidepressant-induced mood cycling.
Bipolar III (3.0)
Patients who develop a manic or hypomanic episode on an antidepressant are sometimes called bipolar III (Figure 6-16). According to formal diagnostic criteria, however, when an antidepressant causes mania or hypomania, the diagnosis is not bipolar disorder, but rather, “substance-induced mood disorder.” Many experts disagree with this designation and feel that patients who have a hypomanic or manic response to an antidepressant do so because they have a bipolar spectrum disorder, and can be more appropriately diagnosed as bipolar III disorder (Figure 6-16) until they experience a spontaneous manic or hypomanic episode while taking no drugs, at which point their diagnosis would be bipolar I or II, respectively. The bipolar III designation is helpful in the meantime, reminding clinicians that such patients are not good candidates for antidepressant monotherapy.
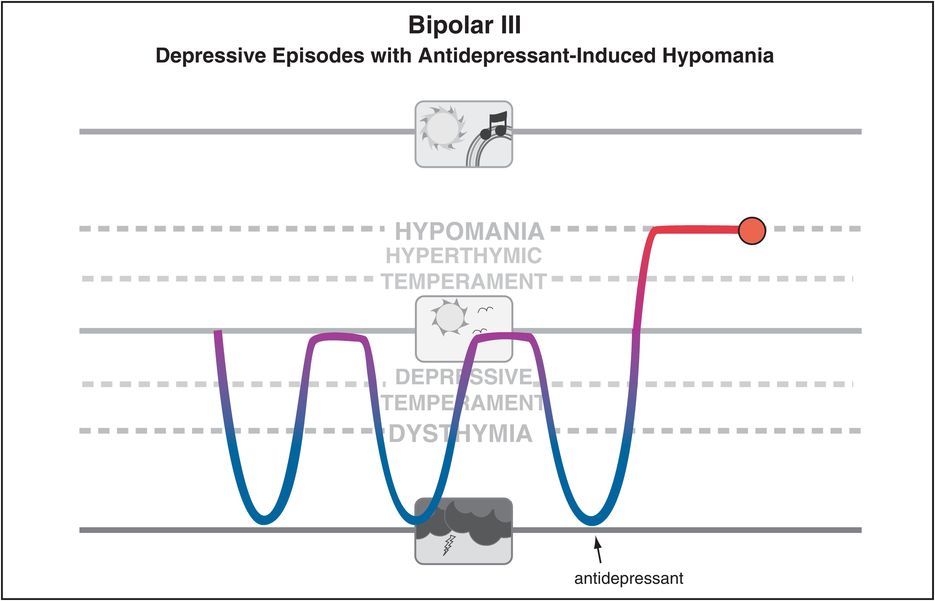
Figure 6-16. Bipolar III. Although the Diagnostic and Statistical Manual of Mental Disorders, fourth edition (DSM-IV), defines antidepressant-induced (hypo)mania as a substance-induced mood disorder, some experts believe that individuals who experience substance-induced (hypo)mania are actually predisposed to these mood states and thus belong to the bipolar spectrum (bipolar III).
Bipolar III½ (3.5)
A variant of this bipolar III disorder has been called bipolar III½, to designate a type of bipolar disorder associated with substance abuse (Figure 6-17). Although some of these patients can utilize substances of abuse to treat depressive episodes, others have previously experienced natural or drug-induced mania and take substances of abuse to induce mania. This combination of a bipolar disorder with substance abuse is a formula for chaos, and can often be the story of a patient prior to seeking treatment from a mental health professional.
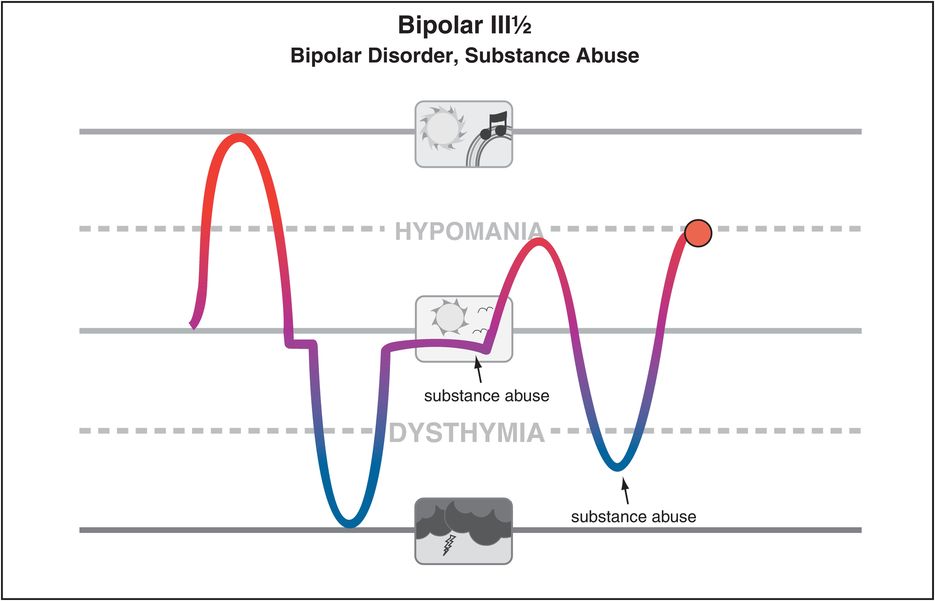
Figure 6-17. Bipolar III½. Bipolar III½ (3.5) is bipolar disorder with substance abuse, in which the substance abuse is associated with efforts to achieve hypomania. Such patients should be evaluated closely to determine if (hypo)mania has ever occurred in the absence of substance abuse.
Bipolar IV (4.0)
Bipolar IV disorder is the association of depressive episodes with a pre-existing hyperthymic temperament (Figure 6-18). Patients with hyperthymia are often sunny, optimistic, high-output, successful individuals with stable temperament for years and then suddenly collapse into a severe depression. In such cases, it may be useful to be vigilant to the need for more than antidepressant monotherapy if the patient is unresponsive to such treatment, or if the patient develops rapid cycling or hypomanic or mixed states in response to antidepressants. Despite not having a formal bipolar disorder, such patients may respond best to mood stabilizers.
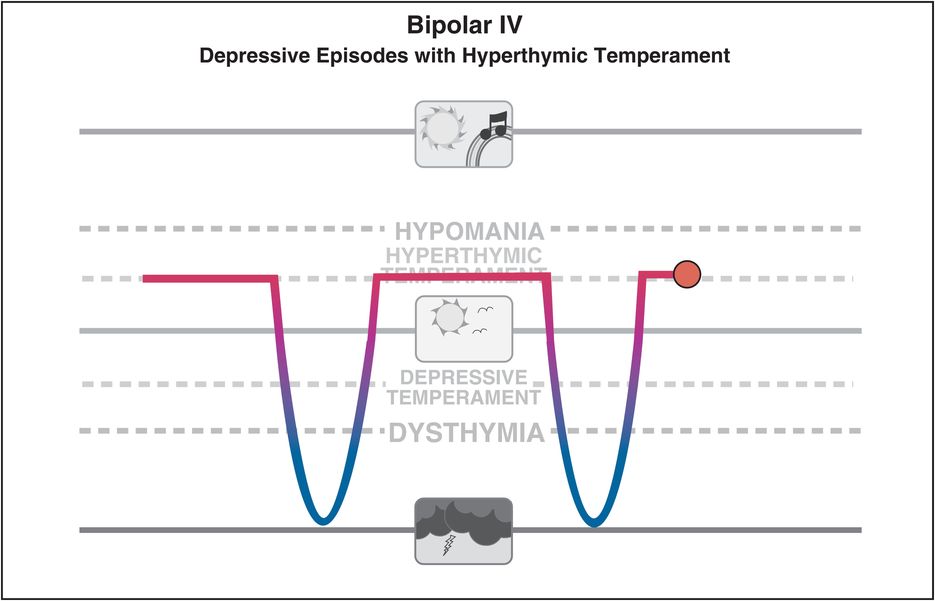
Figure 6-18. Bipolar IV. Bipolar IV is seen in individuals with longstanding and stable hyperthymic temperament into which a major depressive episode intrudes. Individuals with hyperthymic temperament who are treated for depressive episodes may be at increased risk for antidepressant-induced mood cycling, and may instead respond better to mood stabilizers.
Bipolar V (5.0)
Bipolar V disorder is depression with mixed hypomania (Figure 6-19). Formal diagnostic criteria for mixed states require full expression of both depression and mania simultaneously, but in the real world, many depressed patients can have additional symptoms that only qualify as hypomania or subsyndromal hypomania, or even just a few manic symptoms or only mild manic symptoms. Depression simultaneous with full hypomania is represented in Figure 6-1 and Figure 6-5 and requires mood stabilizer treatment, not antidepressant monotherapy. Under debate is whether there should be a separate diagnostic category for depression with subthreshold hypomania; some experts believe that up to half of patients with major depression also have a lifetime history of subsyndromal hypomania, and that these patients are much more likely to progress to a formal bipolar diagnosis. Patients with depression and subthreshold hypomania generally have a worse outcome, more mood episodes, more work impairment, are more likely to have a family member with mania or other bipolar disorder, and to have an early onset of depression. For depression with subsyndromal hypomania it may be more important to emphasize overactivity rather than just mood elevation, and a duration of only 2 days as opposed to the 4 days required in most diagnostic systems for hypomania. Whether these patients can be treated with antidepressant monotherapy without precipitating mania, or instead require agents with potentially greater side effects such as mood stabilizers, lithium, and/or atypical antipsychotics, is still under investigation.
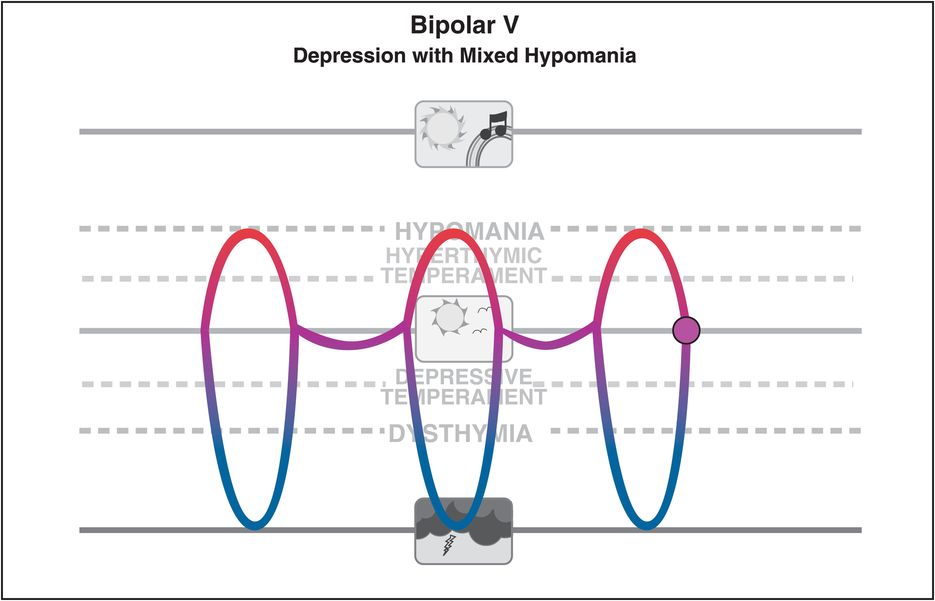
Figure 6-19. Bipolar V. Bipolar V is defined as major depressive episodes with hypomanic symptoms occurring during the major depressive episode but without the presence of discrete hypomanic episodes. Because the symptoms do not meet the full criteria for mania, these patients would not be considered to have a full mixed episode, but they nonetheless exhibit a mixed presentation and may require mood stabilizer treatment as opposed to antidepressant monotherapy.
Related conditions to depression mixed with subsyndromal hypomania include other mood states where full diagnostic criteria are not reached, ranging from full mixed states (both full mania diagnostic criteria [M] and full depression diagnostic criteria [D]) to depression with hypomania or only a few hypomanic symptoms (mD) as already discussed. In addition, other combinations of mania and depression range from full mania with only a few depressive symptoms (Md, sometimes also called “dysphoric” mania), to subsyndromal but unstable states characterized by some symptoms of both mania and depression, but not diagnostic of either (md) (Table 6-1). All of these states differ from unipolar depression and belong in the bipolar spectrum; they may require treatment with the same agents that are used to treat bipolar I or II disorder, with appropriate caution for antidepressant monotherapy. Just because a patient is depressed, it does not mean he or she should start with an antidepressant for treatment. Patients with mixed states of depression and mania may be particularly vulnerable to the induction of activation, agitation, rapid cycling, dysphoria, hypomania, mania, or suicidality when treated with antidepressants, particularly without the concomitant use of a mood stabilizer or an atypical antipsychotic.
| Description | Designation | Comment |
|---|---|---|
| DSM-IV mixed | MD | Full diagnostic criteria for both mania and depression |
| Depression with hypomania | mD | Bipolar V |
| Depression with some manic symptoms | mD | Bipolar NOS |
| Mania with some depressive symptoms | Md | Dysphoric mania |
| Subsyndromal mania and subsyndromal depression | md | Prodrome or presymptomatic state of incomplete remission |
Bipolar VI (6.0)
Finally, bipolar VI disorder (Figure 6-20) represents bipolarity in the setting of dementia, where it can be incorrectly attributed to the behavioral symptoms of dementia rather than recognized and treated as a comorbid mood state with mood stabilizers and even with atypical antipsychotics.
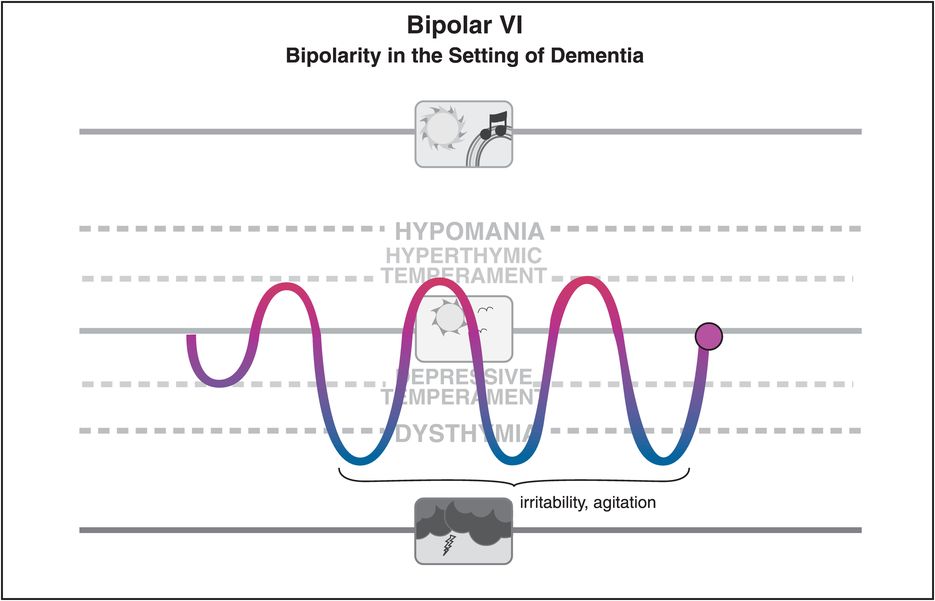
Figure 6-20. Bipolar VI. Another subcategory within the bipolar spectrum may be “bipolarity in the setting of dementia,” termed bipolar VI. Mood instability here begins late in life, followed by impaired attention, irritability, reduced drive, and disrupted sleep. The presentation may initially appear to be attributable to dementia or be considered unipolar depression, but it is likely to be exacerbated by antidepressants and may respond to mood stabilizers.
Many more subtypes of mood disorders can be described within the bipolar spectrum. The important thing to take away from this discussion is that not all patients with depression have major depressive disorder requiring treatment with antidepressant monotherapy, and that there are many states of mood disorder within the bipolar spectrum beyond just bipolar I and II disorders.
Can unipolar depression be distinguished from bipolar depression?
One of the important developments in the field of mood disorders in recent years in fact is the recognition that many patients once considered to have major depressive disorder actually have a form of bipolar disorder, especially bipolar II disorder or one of the conditions within the bipolar spectrum (Figure 6-21). Since symptomatic patients with bipolar disorder spend much more of their time in the depressed state rather than in the manic, hypomanic, or mixed state, this means that many depressed patients in the past were incorrectly diagnosed with unipolar major depression, and treated with antidepressant monotherapy instead of being diagnosed as a bipolar spectrum disorder and treated first with lithium, anticonvulsant mood stabilizers, and/or atypical antipsychotics prior to adding an antidepressant, if an antidepressant is even used at all.
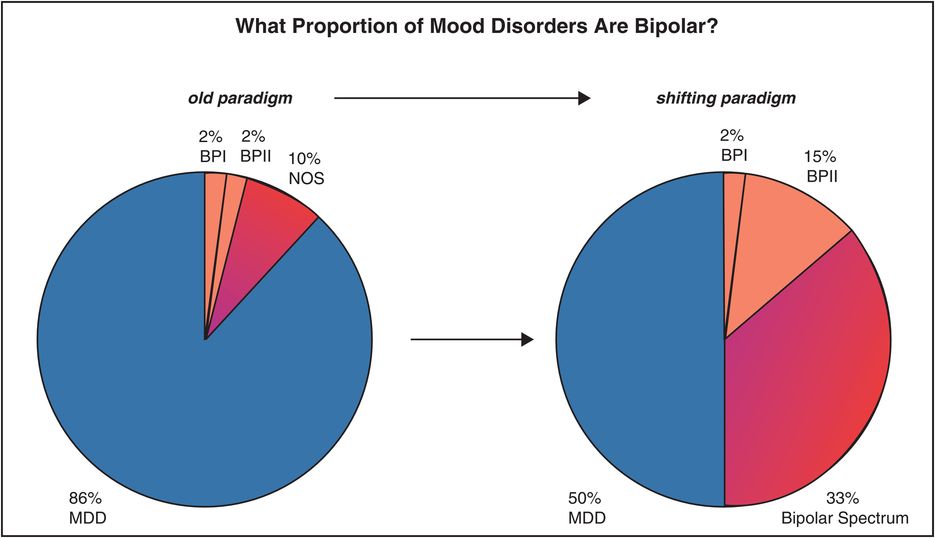
Figure 6-21. Prevalence of mood disorders. In recent years there has been a paradigm shift in terms of the recognition and diagnosis of patients with mood disorders. That is, many patients once considered to have major depressive disorder (old paradigm, left) are now recognized as having bipolar II disorder or another form of bipolar illness within the bipolar spectrum (shifting paradigm, right).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


