Chapter 12 After reading this chapter, the reader will be able to: 1 Describe nutritional disorders and their possible relationship to disorders of other organs 2 Define terminology relating to nutritional disorders 3 Define and describe all bold-faced terms in this chapter 4 Distinguish the pathologic conditions caused by various vitamin deficiencies 5 Describe the pathologic conditions associated with muscular dystrophy, melanoma, and systemic lupus erythematosus 6 Differentiate hereditary abnormalities, including chromosomal aberrations and genetic amino acid disorders Disorders of nutrition range from malnutrition and vitamin deficiency to obesity and hypervitaminosis. In addition to inadequate intake, nutritional deficiency may be related to disorders of the liver, pancreas, and gastrointestinal tract that result in an inability of the body to digest and properly use proteins, carbohydrates, and lipids. In diabetes mellitus, the absence of insulin prevents entry of glucose into the cells and thus deprives the body of its major source of energy. Abnormalities of the pancreas, liver, and gastrointestinal tract that cause nutritional diseases are discussed elsewhere; this section deals with diseases caused by vitamin deficiency, malnutrition, and obesity. Vitamins are an essential part of the enzymatic systems that are vital to the body’s cellular metabolism. Vitamins are formed (synthesized) only by plants, not by animals. Therefore, humans’ supply of vitamins comes directly from eating fruits and vegetables or from animals (including fish) that have eaten plants and have stored the vitamins. Vitamins are generally divided into two categories: fat soluble and water soluble. The fat-soluble vitamins (A, D, E, and K) can be stored within body tissues. Water-soluble vitamins (B and C) cannot be stored and must be a regular part of the diet to prevent a deficiency. The major B vitamins are thiamine, riboflavin, niacin, pantothenic acid, cobalamin (vitamin B12), and folic acid. Vitamin deficiency diseases are rare in the United States but are all too prevalent in underdeveloped countries. Beriberi results from a deficiency in thiamine (vitamin B1), a coenzyme essential for carbohydrate metabolism that promotes growth and maintains muscle tone and heart function. Beriberi occurs primarily in rice-eating countries, such as China, where the main staple is polished rice from which the vitamin-containing skin and germ have been removed. Infantile beriberi is common in breast-fed infants 2 to 4 months of age whose mothers have thiamine deficiency. Noninflammatory degeneration of the myelin sheath caused by thiamine deficiency produces a peripheral neuropathy characterized by weakness of the limbs and a “pins and needles” sensation in the extremities. Radiographic Appearance: Initially, peripheral vasodilatation in beriberi increases cardiac output, which then produces a generalized enlargement of the cardiac silhouette and increased pulmonary vascular markings. With progression of disease, the myocardium becomes edematous and flabby and cannot function properly, leading to congestive heart failure and generalized edema (Figure 12-1). Pellagra, caused by a deficiency of niacin viamin B3), is characterized by reddening and scaling of the skin on exposed parts of the body, vomiting and severe diarrhea, and nervous and mental disorders (ranging from chronic depression to violent, irrational behavior). The body requires niacin to complete the cellular process called respiration, in which nutrients and oxygen reach the cells through a series of chemical reactions. As a result of dietary supplements, epidemics of pellagra no longer exist; however, sporadic incidences occur among chronic alcoholics and people suffering from malabsorption. In patients with scurvy, the deficiency of ascorbic acid vitamin C) leads to an inability of the supporting tissues to produce and maintain vascular endothelium and the cementing substances that hold epithelial cells together (collagen, osteoid, dentin). Scurvy was classically a disease of sailors and explorers deprived of fresh fruit and vegetables containing vitamin C. Radiographic Appearance: In children, disordered chondroblastic and osteoblastic activity cause radiographic bone changes that are most prevalent where growth is normally most rapid (especially about the knee and wrist). The bones are generally osteoporotic with blurring or disappearance of trabecular markings and severe cortical thinning. Widening and increased density of the zone of provisional calcification produce the characteristic “white line” of scurvy (Figure 12-2). A relatively lucent osteoporotic zone forms on the diaphyseal side of the white line. This osteoporotic zone is easily fractured, permitting the dense bone to become impacted on the shaft and to jut laterally beyond it, thus giving rise to characteristic marginal spur formation (Pelken spur). The epiphyseal ossification centers are demineralized and surrounded by dense, sharply demarcated rings of calcification (Wimberger’s sign of scurvy). If epiphyseal dislocations have not occurred, the appearance of the skeletal structures usually returns to normal after appropriate therapy. Rickets is a bone disease of young children in which a lack of vitamin D leads to decreased absorption of calcium from the gastrointestinal tract, resulting in weak, deformed bones. In adults, lack of vitamin D causes generalized softening of bones (osteomalacia). The radiographic findings of rickets and osteomalacia are found in Chapter 4. Excess vitamin D causes too much calcium to be absorbed from the gastrointestinal tract. The resulting hypercalcemia leads to the deposition of calcium in the kidney, heart, lungs, and wall of the stomach (Figure 12-3).
Miscellaneous Diseases
Nutritional diseases
Vitamin Deficiencies
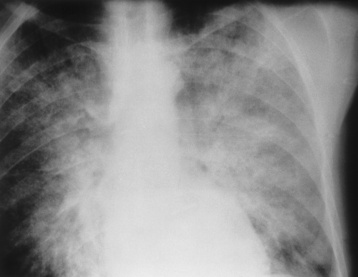
Beriberi (Thiamine Deficiency)
Pellagra (Niacin Deficiency)
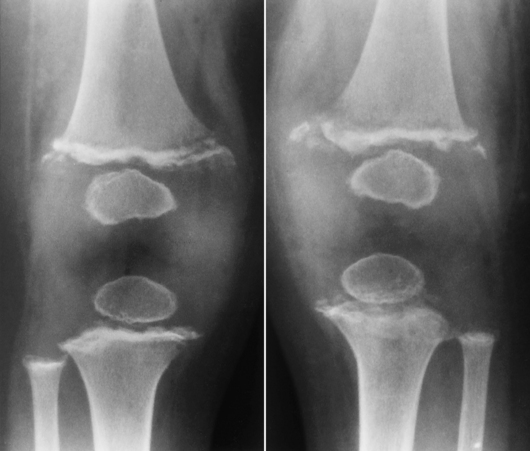
Scurvy (Vitamin C Deficiency)
Rickets (Vitamin D Deficiency)
Hypervitaminosis
Radiographic Appearance
Miscellaneous Diseases