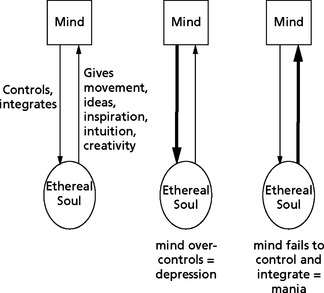
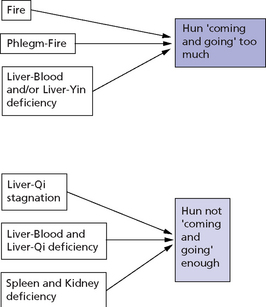
Chapter 44 If the emotional condition is not the presenting problem, I generally ask about a patient’s emotional life towards the end of the consultation to try to find the cause of the disease. In many cases, the emotional state of the patient is the main presenting problem; for example, patients may come to us because they are depressed or anxious. In other cases, the emotional state of the patient is the underlying cause of physical symptoms; for example, a patient may complain of tiredness and digestive symptoms when frustration and resentment may be the cause of the condition. As mentioned above, we must use great sensitivity when asking patients about their emotions. Symptoms and Signs, Chapter 79 Depression is twice as common in women as in men and its onset increases towards middle age. The main symptoms of depression are depressed mood, loss of interest, self-esteem or motivation, fatigue, anxiety, insomnia and loss of appetite. In very severe cases, the patient never comes out of an extremely depressed mood, is unable to experience any pleasure at any time, is in utter despair and may be suicidal. A major depressive syndrome has the following characteristics: In addition to the above manifestations, a major depressive syndrome is also defined by the absence of the following: an organic factor, a normal reaction to bereavement, delusions or hallucinations in the absence of mood symptoms, schizophrenia, delusional disorder, psychotic disorder.1 In fact, the ‘Simple Questions’ in Chapter 71 mentions the Five Stagnations of Wood, Fire, Earth, Metal and Water.2 The ‘Essential Method of Dan Xi’ (Dan Xi Xin Fa, 1347) describes six stagnations of Qi, Blood, Dampness, Phlegm, Heat and Food. It says: ‘When Qi and Blood are harmonized, no disease arises. If they stagnate diseases arise. Many diseases are due to stagnation… stagnation makes things accumulate so that they cannot flow freely, they would like to rise but cannot, they would like to descend but cannot, they would like to transform but cannot … thus the 6 Stagnations come into being.’3 The ‘Complete Book of Jing Yue’ (Jing Yue Quan Shu, 1624) gives stagnation an emotional interpretation and talks about Six Stagnations of anger, pensiveness, worry, sadness, shock and fear. This confirms that all emotions can lead to stagnation of Qi. It says: ‘In the 6 Stagnations, stagnation is the cause of the disease. In emotional stagnation, the disease [i.e. the emotion] is the cause of the stagnation.’4 Figure 44.1 illustrates the two states of the Ethereal Soul: when it ‘comes and goes’ too much; and when it does not ‘come and go’ enough. Essential to the proper movement of the Ethereal Soul is its restraint by the Mind. The Mind (Shen of the Heart) needs to restrain the Ethereal Soul (but not too much) and integrate the material coming from it into the totality of the psyche. If the Mind controls and restrains the Ethereal Soul too much, depression ensues; if the Mind fails to control and restrain the Ethereal Soul, manic behaviours may result (Fig 44.2).
 MENTAL—EMOTIONAL SYMPTOMS
MENTAL—EMOTIONAL SYMPTOMS
WHEN WE ASK
HOW WE ASK
DEPRESSION
Definition of depression
Depression in Chinese medicine
Patterns in depression
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


MENTAL—EMOTIONAL SYMPTOMS