Chapter 25 Menopause
Introduction
The definition of menopause is when there is no menstruation over a 12-month period. That is, when menstrual periods permanantly stop. Women undergo significant reproductive transitional and physiological changes which are accompanied by the additional effects of ageing and social adjustment. This phase known as the climacteric or perimenopause describes the time leading up to a woman’s final menstruation, along with the endocrinological, biological, and clinical features of the approaching menopause. The length of this transition is usually about 4 years, but is shorter in smokers than non-smokers.1 Ten percent of women may not experience this phase and menses may stop abruptly. The median age for menopause is 51 years, over an age range of 39–59 years.1, 2
This transitional phase is associated with a number of vasomotor, urinary symptoms and psychological tribulations (Table 25.1). There is a variation in symptoms experienced.
Table 25.1 Physical, vasomotor and urogenital symptoms, and psychological problems encountered by women approaching and during menopause
| Physical/vasomotor symptoms | Urogenital symptoms | Psychological problems |
|---|---|---|
| Hot flushes | Loss of confidence | |
| Night sweats | Depressed mood | |
| Palpitations | Lack of libido | Irritability/anxiety |
| Headaches | Forgetfulness | |
| Amenorrhoea | Difficulty in concentrating | |
| Dry skin | Panic attacks | |
| Hair loss | Insomnia | |
| Joint pains | Fatigue | |
| Breast tenderness | ||
The severity of symptoms that women may experience range from mild to severe. Approximately 40–65% of women experience hot flushes or night sweats, 30–60% disturbed sleep, and 25–35% vaginal dryness which leads women to consult health professionals.3 The duration of these symptoms may vary from 2–20 years.4
The most effective treatments for hot flushes include oestrogens and progestagens.2 Current evidence supports short-term use of hormone replacement therapy (HRT) as the standard therapy for hot flushes.5, 6 Since the Women’s Health Initiative and Millenium study findings with long-term use of HRT in menopausal women, demonstrated increased risk of breast cancer7 more women are turning to non-pharmacological and various complementary medicines (CMs) for the relief of menopausal symptoms. Many women are reluctant to accept hormonal treatments, except when symptoms are severe, as they see this stage of their lives as a natural event, and not a disease. Menopause is an opportunity for lifestyle changes and it is worthwhile exploring prevention strategies, as women who commence HRT for hot flushes are likely to re-experience them after stopping HRT, even after 5 years.8
Lifestyle changes
Reduced physical activity, low socioeconomic status and cigarette smoking (past and current) are contributors documented to increase the relative risk of hot flushes in menopausal women.9 A recent review has reported that lifestyle and diet adjustment interventions have the potential to significantly improve menopausal symptoms.10, 11 Hence, lifestyle behaviours are important determinants of menopausal symptoms. The available literature suggests that smoking and greater body weight are risk factors for vasomotor symptoms; women with vasomotor symptoms who smoke may benefit from smoking cessation, and women who are heavier than ideal body weight may benefit from weight reduction.12
Body mass/overweight
Very obese women have significantly higher odds of experiencing hot flushes compared with normal weight women. Whilst the mechanism is not clear, oestrogen levels may partly explain this relationship.13
Cigarette smoking
A case-control study of 611 middle-aged women (45–54 years) demonstrated that past and current smokers have higher odds of experiencing hot flushes compared with never smokers.14 Past and current smoking and duration of smoking influenced frequency and the severity of hot flushes. The longer the women smoked, the more severe the symptoms. Smoking did not influence blood levels of estradiol and estrone and the risk persisted even when women were treated with hormones. Cigarette smoking is therefore a strong predictor of experiencing hot flushes, including the severity of hot flushes.
Cultural differences
There are many cultures where the prevalence of menopausal symptoms is reported as low. Prevalence rates for vasomotor symptoms in surveys of women (on average 2-week recall of symptoms) conducted between 2000–2005 include:15 of interest, the lowest reported symptoms are found in peasant Greek women and Mayan women from Mexico.15, 16
Under-reporting of symptoms by women in surveys may also contribute to low prevalences. It is not clear why the incidence of menopausal symptoms vary in different geographical areas. A recent review has reported that the prevalence variation of these symptoms may be influenced by a range of factors, including climate, diet, lifestyle, women’s roles, and attitudes regarding the end of reproductive life and ageing.17 Women’s attitude and expectations that can influence the experience of the perimenopause are determined by a number of factors including cultural attitudes and expectations, medicalisation (menopause viewed as an illness), their reproductive history, general health, mother’s experience, marital status, relationships with and attitude by their husbands/partners, extended family, social support, career and religious belief. In general, a healthy lifestyle, namely diet (e.g. foods high in phytoestrogens and isoflavones), exercise and avoiding smoking, and strong support from friends and family can positively impact on menopausal symptoms.15
| negligible | |
| 15.1% | |
| 17.6% | |
| 23% | |
| 22–46.6% | |
| 36.6–37.8% | |
| 46.5% | |
| 26.2–44.7% | |
| 49% | |
| 55% | |
| 61% |
Health practitioners and other caregivers should recognise that variations exist and ask patients specific questions about symptoms and their impact on usual functioning.17–20
Core body temperature
Possible mechanisms for hot flushes include the effects of oestrogen on norepinephrine/noradrenaline and serotonin receptors in the hypothalamus21 and genetics may also play a role.22 Research evidence suggests that small temperature elevations preceding hot flushes may constitute a triggering mechanism.20, 23 In addition, higher body core temperature prior to and during sleep is significantly associated with poorer quality of sleep and higher luteinizing hormone (LH) levels.24
Mind–body medicine
Psychological support
In a study of 78 menopausal women suffering hot flushes and breast cancer, the women were randomised to education and psychosocial support groups or a control group.25 A significant improvement in symptoms was found with the active treatment.25 A recent pilot trial demonstrated a possible effectiveness of cognitive behavioural interventions for the treatment of climacteric syndrome.26 A further pilot investigating cognitive behavioural group therapy (CBGT) supported the notion that CBGT interventions aimed at reducing vasomotor symptoms may be of value for menopausal hot flushes when administered in a small-group format.27 A recent systematic review has concluded that psycho-educational interventions seem to alleviate hot flushes in menopausal women and breast cancer survivors.28
Relaxation therapies
Nervous tension may cause instability of the thermoregulatory centre leading to sudden, transient, and erratic peripheral vasodilation in the skin blood vessels causing the sensation of flushing.29 Interestingly, even excitement, such as laughter, can stimulate the nervous system and bring on more hot flushes. Relaxation can alleviate menopausal symptoms.28
Three randomised control trials (RCTs) identified by the North American Menopausal Society,30 demonstrated paced respiration (slow, controlled, diaphragmatic breathing) reduced hot flushes by 50%, particularly if performed at the onset of a hot flush when compared with controls. A pilot study of mindfulness-based stress reduction for hot flushes has shown a positive result in improving both quality of life and reducing severity of hot flushes in 15 women experiencing severe hot flushes over the course of treatment.31
Physical activity/exercise
Aerobic exercise and customised exercise programs
Physical activity may ameliorate hot flushes and insomnia by influencing opioid levels.32 It is known that opioid levels are lowered in menopause and that exercise can increase opioid levels such as endorphins and activity.33 Although data supporting physical activity are still preliminary recent studies suggest that women who exercise regularly are less likely to experience severe hot flushes.34 A customised exercise program is valuable for improving the health related quality of life of menopausal women compared to those who do not perform any form of physical activity.35
A Cochrane review of RCTs identified 1 small trial that compared exercise with HRT and found both interventions were effective in reducing vasomotor symptoms, although HRT was more effective than exercise.36
A recent systematic review of the literature of RCTs found aerobic exercise improves psychological health and quality of life in vasomotor symptomatic women.37 The review also identified several RCTs of middle-aged menopausal women and found aerobic exercise can invoke significant improvements in this age group of menopause-related symptoms such as mood, health-related quality of life and insomnia compared with middle-aged women who did not exercise.37
Yoga
Yoga can play an important role in the management of menopausal symptoms. A number of trials support the recommendation of specific yoga exercises as an evidence-based prescription for menopausal symptoms.38, 39, 40
A recent randomised control study of 180 perimenopausal women comparing yoga comprised of breathing practises, sun salutation and meditation was found to be significantly beneficial for reducing hot flushes and night sweats and improving cognitive functions such as memory, mental balance, attention, concentration and recall when compared with control group; a set of simple physical exercises, under supervision.41
A trial of 120 women (aged 40–55 years) with menopausal symptoms randomised women into 2 study arms: yoga and an exercise (control) group.42 In the yoga therapy group, women were instructed to practise various yoga postures such as sun salutation that consists of 12 postures, pranayama (breathing practices) and avartan dhyan (cyclic meditation). Women in the control group were instructed a set of simple physical exercises (supervision by trained teachers). Women in both groups practised either yoga or physical exercises 1 hour daily, 5 days per week over the 8-week study period.
The perimenopausal women in the yoga therapy group demonstrated significantly reduced perceived stress, climacteric symptoms, and neuroticism traits compared with controls.42
A systematic review that explored the role of meditation and yoga for treating diseases concluded the strongest evidence for efficacy was found for epilepsy, symptoms of the premenstrual syndrome and menopausal symptoms.43
However, a recent systematic review of 7 studies reported mixed results and the evidence at present is insufficient to suggest that yoga is effective in menopause.44
Some studies did not demonstrate any benefit of yoga on menopausal symptoms, sleep or self-esteem in menopausal women.44, 45, 46
Nutritional influences
Calcium and vitamin D for menopausal women
There is a role for the recommendation of calcium and vitamin D (cholecalciferol) supplementation by menopausal women with demonstrated vitamin D deficiency for the prevention of osteoporosis. Routine use, however, is questionable. (See Chapter 30 for osteoporosis.)
A Cochrane review of 45 trials, found vitamin D alone is not effective in preventing hip fracture, vertebral fracture or any new fracture.47 Vitamin D with calcium reduced hip fractures especially in people in institutional care, but not significantly in the community-dwelling subgroup.47
The World Health Initiative for the calcium/vitamin D RCT of 36 282 post-menopausal women (aged 51–82 years) from 40 US clinical centres assigned to 1000mg of elemental calcium carbonate and 400IU of vitamin D(3) daily or placebo with average follow-up of 7 years, found that supplementation did not have a statistically significant effect on mortality rates but may reduce mortality rates in post-menopausal women.48
Furthermore, findings from the Women’s Health Initiative study also found adherence to calcium and vitamin D supplements over 4 years did not produce any favourable effects compared to placebo on physical functioning or physical performance in the older women.49
Phytoestrogens and isoflavones in diet
Phytoestrogens are oestrogenic compounds found in plants and consist of isoflavones, lignans and coumestans (Table 25.2).50 Isoflavones have a similar structure to oestrogen and have the capacity to exert both mild oestrogenic effects in menopausal women and anti-oestrogenic effects in pre-menopausal women.50 Comparative surveys of Japanese women and parallel groups of women from Canada and North America determined significant differences in the incidence of hot flushes and nocturnal sweating during premenopausal, perimenopausal and post-menopausal phases.51
Table 25.2 Foods rich in phytoestrogen content
| Phytoestrogen food sources | Phytoestrogen content (μg/100g) |
|---|---|
| Flax seed | 379380 |
| Soy beans | 103920 |
| Tofu | 27150.1 |
| Soy yoghurt | 10275 |
| Sesame seed | 8008.1 |
| Flax bread | 7540 |
| Black bean sauce | 5330.3 |
| Multigrain bread | 4798.7 |
| Soy milk | 2957.2 |
| Hummus | 993 |
| Soy bean sprouts | 789.6 |
| Garlic | 603.6 |
| Mung bean sprouts | 495.1 |
| Dried apricots | 444.5 |
| Alfalfa sprouts | 441.4 |
| Pistachio nuts | 382.5 |
| Dried dates | 329.5 |
| Sunflower seed | 216 |
| Chestnuts | 210.2 |
| Dried prunes | 183.5 |
| Olive oil | 180.7 |
| Walnuts | 139.5 |
| Almonds | 131.1 |
| Green beans | 105.8 |
| Broccoli | 94.1 |
| Cabbage | 80 |
| Peaches | 64.5 |
| Strawberry | 51.6 |
| Peanuts | 34.5 |
| Onion | 32 |
| Blueberry | 17.5 |
| Corn | 9 |
| Coffee with cow’s milk | 6.3 |
| Watermelon | 2.9 |
| Milk, cow | 1.2 |
(Source: adapted and modified from Thompson LU, Boucher BA, Lui Z, et al. Phytoestrogen content of foods consumed in Canada, including isoflavones, lignans and coumestan. Nutrition and Cancer 2006; 54:184–201.)
However, a diet high in phytoestrogens alone is probably less successful in addressing menopausal symptoms without a change in lifestyle and more physical activity as well as the awareness of a low-calorie diet and stress management. This notion was evident in a cross-cultural comparison of health-related quality of life in Australian and Japanese midlife women.52 It was reported that if the women had a lowered body mass index, undertook physical activity, consumed dietary phytoestrogens, and consumed some alcohol (any regular use of alcohol) their physical functioning seemed to be better.52
Asians and Japanese ingest on average 25–45mgs isoflavones per day over long periods of time. Just 40mg of isoflavones alone is sufficient to reduce menopausal symptoms which are up to 50 000 times higher than levels of endogenous estradiol.15
Furthermore, a high-phytoestrogen diet especially if initiated before puberty is associated with reduced risk of breast, colon and prostate cancer.53, 54
Middle-aged Japanese women are generally healthier than North American women, have lower rates of heart disease, breast cancer and osteoporosis, and have one of the longest life expectancy in the world (mean 85.33 yrs).51
The incidence of breast cancer is one-third compared with North American women, for osteoporosis less than half of Caucasian women in North America, even though Asian women have lower bone density, and 28% suffer a chronic health problem such as diabetes, allergies, asthma, arthritis and hypertension compared with 45% of Canadian (Manitoban) women and 53% of US (Massachusetts) women.15
The authors attribute these results to exercise, including weight-bearing exercise, no smoking, minimal consumption of alcohol and coffee, and a low-fat diet high in soybeans, vegetables and herbal teas (phytoestrogen-rich).15
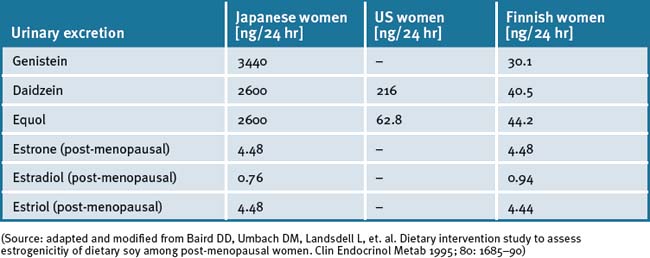
Comparative studies of Japanese-oriental women, US and Finnish women proved that the Japanese women had a 60 to 110 times higher amount of isoflavones excreted in the urine while the concentration of oestrone and oestradiol was nearly identical and the amount of oestradiol was slightly less.55 The average age in both groups (Japan and Finland) was 50.4 years. Both groups came from rural regions, therefore the socio–psychological differences were less than assumed. The measured higher concentrations of isoflavones in Japanese women were attributed to high consumption of soy products such as tofu, miso, aburage, atuage, koridofu as well as cooked soy beans. It was concluded that this dietary factor was responsible for less climacteric complaints and protective effect against cancer. (See Table 25.3.)
Table 25.3 Excretion of isoflavones, phystoestrogens, and endogenous oestrogens in Japanese, American and Finnish women (with Western-type nutrition)
Nutritional supplements
Phytoestrogens
Safety concerns with the use of phytoestrogen supplements have been raised,56 but the general consensus is that they are safe except where there is still uncertainty in some situations such as in women with breast cancer.57 Phytoestrogens can also competitively bind to oestrogen receptors, displacing more potent oestrogens, and potentially decrease the overall oestrogenic effect in the premenopausal woman.58
Recent evidence demonstrates that a high dietary soy intake in women with a history of oestrogen and progesterone positive receptor breast cancer, had a significantly lower risk of breast cancer recurrence while taking tamoxifen.59
Soy (Glycine max L.) isoflavone extracts
A randomised double-blind, placebo-controlled trial has demonstrated that supplementation of soy isoflavones up to 100mgs/day for 4 months in post-menopausal women reduced cholesterol and menopausal symptoms by 21%.60
In another RCT, 25g of soy protein alone was able to reduce total cholesterol and LDL-cholesterol (-29.0 and -24.0mg/dL, p<0.001 and p<0.006) after 16 weeks compared with placebo and resistance exercise.61
Other studies have demonstrated its effectiveness only when the diet involved increasing phytoestrogen intake. Murkies et al.62 demonstrated that after 3 months, the soy flour supplementation evidenced a 40% reduction in hot flushes compared with controls fed wheat flour resulting in only 25% reduction. Advising patients to add 2 tablespoons of soy grits to their diet, such as cereal, may be comparable.
A double-blind, randomised, placebo-controlled study of 80 post-menopausal women (mean age = 55.1 years), who reported 5 or more hot flush episodes per day, were randomised to receive either 250mg of standardised soy extract (Glycine max AT) a total of 100mg/day of isoflavone or placebo.63
A 12-week randomised placebo-controlled trial of 84 post-menopausal women randomised to 20g of soy protein containing 160mg of total isoflavones or taste-matched placebo (20g whole milk protein) demonstrated a significant improvement in all 4 quality-of-life subscales (vasomotor, psychosexual, physical, and sexual) among the women taking isoflavones compared with no changes observed in the placebo group.64
Another study has also demonstrated efficacy and safety of a soy isoflavone extract in post-menopausal women.65 The soy isoflavone extract exerted favourable effects on vasomotor symptoms and compliance was good, providing a safe and effective alternative therapy for post-menopausal women.
However, RCTs have yielded mixed results for the effectiveness of soy isoflavones for menopausal symptoms due to various factors such as small sample sizes, short-term treatment and variation in dosage used. In addition, there is sub-population and individual variation in the metabolisation of daidzein which converts to the more bioactive estrogenic product equol by the gut bacteria. Western women are only 30% equol producers compared with 50–60% of Japanese women.15
A recent Cochrane review66 concluded that there was no evidence of effectiveness in the alleviation of menopausal symptoms with the use of phytoestrogen treatments.
Yet another systematic review and meta-analysis of multiple RCTs using a non-random effects model, demonstrated that isoflavone therapy had a significant 30% reduction in frequency hot flushes, especially in women with frequent hot flushes.67
Interestingly it has also been reported that the quality of soy phytoestrogens is almost certainly likely to influence efficacy.68
Herbal medicine
Herbal medicines may play a role in short-term management of the symptoms of menopause.
A review of the literature found the majority of studies indicate that extract of black cohosh (Cimicifuga racemosa) improves menopause-related symptoms, although the quality of studies is poor.69 Studies for isoflavone red clover (Trifolium pratense L.) leaf extracts to relieve menopausal symptoms are contradictory. When compared with placebo, the largest study showed no benefit for reducing menopausal symptoms for 2 different red clover isoflavone products.69 Clinical trials for the use of dong quai (Angelica sinensis L.), ginseng (Panax ginseng), or evening primrose seed oil (Oenothera biennis L.) demonstrate these are ineffective for improving menopausal symptoms.69
Another review suggests that isoflavones found in soy foods and red clover appear to have a ‘small but positive health effect on plasma lipid concentrations, bone mass density, and cognitive abilities’.70
Red clover (Trifolium pratense)
Red clover is a member of the legume family and contains high levels of isoflavones, namely genistein, and significantly less daidzein compared with soy. Daidzein converts to the more bioactive equol, which exerts stronger estrogenic effects, and may explain why red clover is less effective than soy extracts in clinical trials.71, 72
The majority of placebo–controlled, randomised, double-blind studies have resulted in no effect of 40–160mg isoflavones (red clover isoflavones).73, 74
Three blinded randomised trials with red clover supplements containing either 57mgs/day isoflavones or 40mgs/day isoflavones found no benefit for hot flushes in peri- and post-menopausal women.75 A further trial of 30 women aged 49–65 years, after 4 weeks, reported reduced hot flushes with 80mgs/day of red clover propriety extract compared with placebo.76 Another similar trial demonstrated red clover to reduce symptoms of menopause with up to 73% of women experiencing a significant improvement, 50% reduction of hot flushes and 47% reduction in night sweats within 6 weeks of treatment.76 However, a systematic review identified 5 trials measuring the effects of T. pratense isoflavones on vasomotor symptoms in menopausal women.77 The meta-analysis only indicates a small reduction in hot flush frequency in women receiving active treatment (40–80mg/day) compared with those receiving placebo. A recent, large US clinical trial concluded that the red clover extract had no clinically important effect on hot flashes or other symptoms of menopause.78
A more recent systematic review and meta-analysis confirms efficacy of red clover extract.79 It was concluded that there was evidence (albeit small) from T. pratense isoflavones for treating hot flushes in menopausal women. Minimal side-effects and no serious safety concerns were associated with short-term use of red clover, although technically one would avoid its use in estrogenic related health problems such as breast and endometrial cancers due to its high oestrogenic content, although this is not well established. A double-blinded placebo-controlled trial of 30 perimenopausal women demonstrated no proliferative effects on the endometrium by biopsy after 12 weeks of use with red clover-derived isoflavone extract, suggesting it may possibly have an anti-oestrogenic effect on the uterus.80 A recent review of the literature confirms this finding.81 Red clover demonstrates some efficacy in maintenance of bone health and improvement of arterial compliance.82
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


