Chapter 1 Medical record, medical history and interviewing technique
CONSULTATION, MEDICAL HISTORY AND RECORD-TAKING
The ability to take an accurate medical history from a patient is one of the core clinical skills and an essential component of clinical competence. The success of the medical consultation depends not only on the doctor’s clinical knowledge and interview skills but also on the nature of the relationship that exists between doctor and patient. Patients need to feel sufficiently at ease to disclose their problems and express their concerns, and to know they have been understood by the doctor. Patients also need to reach a shared understanding with the doctor about the nature of their illness and what is proposed to deal with it.
INTERVIEWING TECHNIQUES AND HISTORY-TAKING
The medical consultation is the main opportunity for the doctor to explore the patient’s problems and concerns and to start to identify the reasons for the patient’s ill health. Models of history-taking are becoming more patient-centred and seeking to assess both main components of ill health – the biomedical component and the psychosocial component.
STARTING THE CONSULTATION
Identifying the patient’s problems and concerns
Begin by asking patients to outline their problems and concerns by using an open-ended question (e.g. ‘Tell me what has brought you to the doctor today’). Remember patients may have more than one concern they wish to raise and discuss. The order of their problems may not relate to their importance from either the patient’s or doctor’s perspective. It is therefore particularly important in this opening phase not to interrupt the patient in case this inhibits the disclosure of important information.
GATHERING INFORMATION – THE HISTORY
Biomedical perspective
 Symptoms and signs: Five fundamental questions you are trying to extract for the history
Symptoms and signs: Five fundamental questions you are trying to extract for the history Symptoms and signs: Pain assessment
Symptoms and signs: Pain assessmentBackground information
The information that is gathered about a patient’s problems needs to be set in the context of the individual. Contextual information requires enquiry into a person’s family history, personal and social history, past medical history and drug and allergy history.
Family history
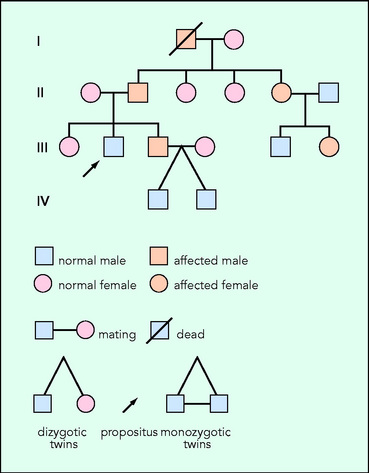
Ask about any disorders that might be inherited, social partnerships (e.g. does the patient have a regular partner, is the patient married) and children. It may be helpful to construct a family tree (Fig. 1.1).
Personal and social history
Enquire about education, employment (past and present – is there suspicion of exposure to an occupational hazard?), social support networks, home circumstances (does the patient live alone? Can the patient attend to his or her personal needs – bathing, cooking? Are there financial worries?).
Also at this point ask about tobacco and alcohol.
 Symptoms and signs: Units of alcohol equivalents (approximate)
Symptoms and signs: Units of alcohol equivalents (approximate)


