Measles Pneumonia
Key Facts
Etiology/Pathogenesis
Causative agent is a single-stranded, enveloped virus of the family Paramyxoviridae, genus Morbillivirus
Clinical Issues
Exposure in children < 6 years of age usually results in lifelong immunity
Pulmonary complications usually occur in immunocompromised or debilitated patients and may progress to fatal pneumonia
Microscopic Pathology
Necrotizing bronchiolitis with extensive destruction of epithelial lining of bronchioles
Squamous metaplasia of bronchial and bronchiolar lining epithelium
Giant cell interstitial pneumonia with numerous multinucleated epithelial giant cells
Interstitial mononuclear inflammatory cell infiltrate
Abundant intraalveolar exudate with hyaline membrane formation indistinguishable from DAD
Giant cells can show up to 60 nuclei and are prominently enlarged (up to 100 µm in diameter)
Multinucleated giant cells contain homogeneous, small eosinophilic intranuclear and cytoplasmic inclusions
Ancillary Tests
Presence of virus can be confirmed by immunohistochemistry using specific measles antibodies
Viral particles can be identified in cells by using specific probes by DNA in situ hybridization
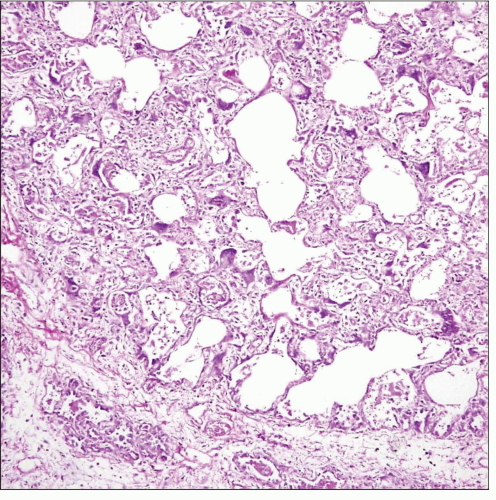 Histological appearance on scanning magnification of giant cell interstitial pneumonia in a patient with measles infection shows expansion of alveolar walls by mononuclear cell infiltrate admixed with giant cells. |
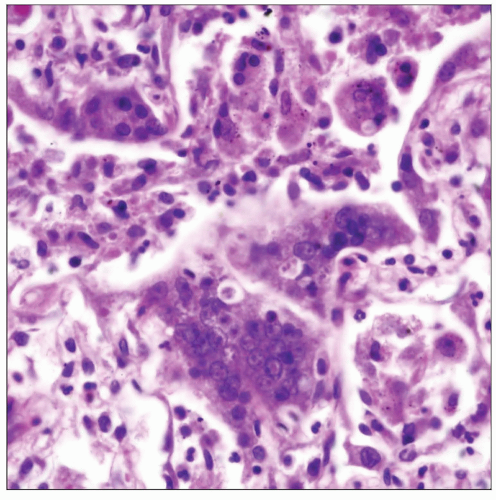 Higher magnification of the infiltrate in giant cell interstitial pneumonia due to measles shows multinucleated giant cells containing abundant small, uniform nuclei surrounded by inflammatory cell infiltrate. |
TERMINOLOGY
Definitions
Highly contagious pulmonary infection caused by measles virus (rubeola)
ETIOLOGY/PATHOGENESIS
Infectious Agents
Causative agent is a single-stranded, enveloped virus of the family Paramyxoviridae, genus Morbillivirus
Virus is spread by aerosols and droplets from respiratory secretions of acute cases
CLINICAL ISSUES
Epidemiology
Incidence
Worldwide infection, particularly prevalent in underdeveloped countries
Recrudescence has occurred in some urban areas of USA due to diminished use of vaccine
Mortality is 1 in 1,000 patients
Age
Children and young adults
Presentation
Prodromal period consists of fever, cough, rhinorrhea, and conjunctivitis, with Koplik spots in buccal mucosa
Erythematous maculopapular rash develops 3 days after onset and involves the face, trunk, and extremities
Pulmonary complications include secondary pneumonia, giant cell pneumonia, and atypical pneumonia
Natural History
Exposure in children < 6 years of age usually results in lifelong immunity
Most adults have lifelong immunity either due to vaccination or previous exposure
Clinical infection has incubation period of 1-2 weeks followed by prodromal period and skin rash
Symptoms usually resolve spontaneously over period of days with complete resolution
Pulmonary complications usually occur in immunocompromised or debilitated patients and may progress to fatal pneumonia
Treatment
Drugs
Immune globulin may be helpful if administered within 1st week of exposure
Prognosis
Measles pneumonia can be fatal in immunocompromised patients
IMAGE FINDINGS
Radiographic Findings
Bilateral fine reticular opacities and patchy consolidation throughout the lungs
CT Findings
Ground-glass opacities, small nodules, and consolidation
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


