Male Reproductive System
Bungo Furusato
Isabell A. Sesterhenn
▪ Questions and Answers
1. A 35-year-old man detected a small nodule in his left scrotum (Fig. 11.1). Which is the correct diagnosis?
a. Adenomatoid tumor
b. Sertoli cell tumor
c. Malignant mesothelioma
d. Metastatic adenocarcinoma
e. Yolk sac tumor
View Answer
1. a. Adenomatoid tumor is a common paratesticular tumor involving the epididymis, tunica, and, rarely, the spermatic cord. These tumors can be found in association with the uterus, fallopian tubes, ovaries, and retroperitoneum adjacent to the adrenal. Histologically, the tumor consists of fibrous stroma with varying amounts of smooth muscle and inflammatory infiltrate. The epithelial cells are mesothelial in origin and form solid strands or cords. The cytoplasm contains vacuoles, which often coalesce resulting in cystic spaces with a “spider web” appearance.
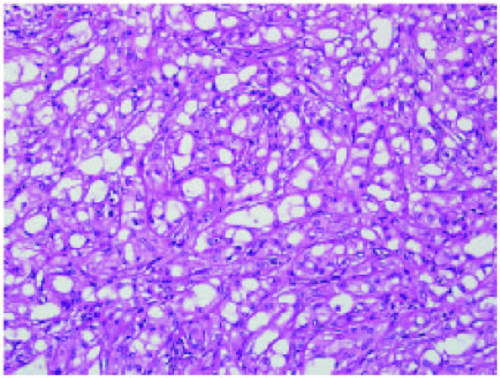 Figure 11.1 |
2. What is the normal upper limit for alpha-fetoprotein (AFP) in the adult?
a. 2 µg/mL
b. Up to 4.5 µg/mL
c. Up to 9 µg/mL
d. Less than 1 µg/mL
e. Not detectable
3. In a patient with mixed germ cell tumor containing 40% or more of embryonal carcinoma, with vascular invasion and with clinical stage I disease, what is the frequency of microscopic metastases to the retroperitoneal lymph nodes at the time of orchiectomy?
a. Never in clinical stage I
b. Less than 2%
c. Approximately 5%
d. Approximately 13%
e. Approximately 30%
View Answer
3. e. In this setting, there is a 30% chance of having retroperitoneal metastasis. In a mixed germ cell tumor with more than 40% of embryonal carcinoma and vascular or lymphatic invasion, the likelihood of stage II disease increases.
4. What is the most common germ cell tumor in prepubertal boys?
a. Seminoma
b. Yolk sac tumor
c. Teratoma
d. Leydig cell tumor
e. Embryonal carcinoma
View Answer
4. b. Yolk sac tumors account for up to 60% of germ cell tumors in infants and children.
5. Which serum level of AFP would you expect in a patient with this germ cell tumor (Fig. 11.2)?
a. 30 µg/mL
b. Up to 9 µg/mL
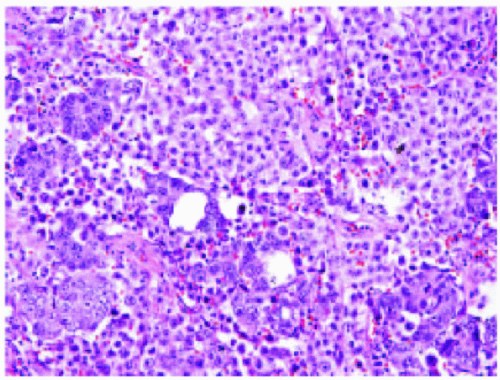 Figure 11.2 |
c. 520 µg/mL
d. 150 µg/mL
e. 3000 µg/mL
View Answer
5. b. Elevated serum levels of AFP are generally due to the presence of yolk sac tumor either in pure form or in association with other germ cell tumor types. AFP production is also seen in glandular or in hepatoid elements of teratoma. About 13% of embryonal carcinomas may show AFP production in isolated or small groups of tumor cells and are not associated with detectable serum level elevations. Seminoma is generally negative for this marker histologically and serologically.
6. A 2-year-old boy has an orchiopexy for an inguinal testis. The pediatrician would like to know what is the risk of developing a germ cell tumor?
a. Less than 15%
b. Approximately 30%
c. Approximately 40%
d. Approximately 90%
e. None of the above
View Answer
6. a. The patient with cryptorchidism has a 3 to 5 times increased risk of developing testicular cancer. Therefore, the lifetime probability of developing a germ cell tumor is approximately 3.5% to 14%.
7. A 28-year-old patient had a right orchiectomy for stage I nonseminomatous mixed germ cell tumor (NSGCT) confirmed by pathology. What is the chance of having or developing a germ cell tumor in the opposite testis?
a. Approximately 20%
b. Approximately 35%
c. Approximately 4%
d. Approximately 57%
e. None of the above
View Answer
7. c. The patient has a 2% to 5% chance of having a contralateral tumor and has a more than 20-fold increased risk for tumor development compared with the general population. Intratubular germ cell neoplasia can be identified in about 5% to 6% in the contralateral testicular biopsy. It is important to teach patients about tes – ticular tumors to perform regular self-examination of the contralateral testis.
8. What other disease can cause an increased serum level of human chorionic gonadotrophin (HCG)?
a. Lung cancer
b. Prostate cancer
c. Colon cancer
d. All of the above
e. None of the above
View Answer
8. d. Ectopic HCG production can be seen in any malignancy, particularly carcinomas. Such tumors often have marked nuclear anaplasia. The ectopic HCG production can cause elevated serum levels of HCG. Other placental glycoproteins (e.g., human placental lactogen, PLAP, etc.) can also be identified in nongerm cell tumors.
9. What type of genetic disorder is associated with the large cell calcifying Sertoli cell tumor?
a. Carney syndrome
b. Gardner syndrome
c. Angelman syndrome
d. Beckwith-Wiedemann syndrome
e. None of the above
View Answer
9. a. Carney syndrome is a rare disorder characterized by mucocutaneous pigmentation, atrial myxoma, endocrine tumors (pituitary, adrenals), and large cellcalcifying Sertoli cell tumors. The latter are often bilateral and consist of large eosinophilic cells resembling Leydig cells. The cells form cords or tubules. The calcifications vary in extent. Some of these tumors are malignant.
10. A 65-year-old man presented with a testicular mass. Radical orchiectomy was performed. The histology was consistent with spermatocytic seminoma. Which of the following statements correctly describes this entity?
a. It is regarded as the testicular tumor of older men.
b. It is not reported in children, cryptorchid testis, or extratesticular sites.
c. It contains three cell types: abundant intermediatesized cells, small lymphocyte-like cells, and larger cells.
d. It does NOT show elevation of AFP or HCG.
e. All of the above.
View Answer
10. e. Spermatocytic seminoma is a rare neoplasm comprising about 2% to 5% of testicular germ cell tumors. There is no correlation with cryptorchidism. It usually arises in older men around age 50 to 55 and has not been reported in prepubertal children or adolescents. It has not been reported in extratesticular sites, or in association with other germ cell tumors. Clinically, most patients present with painless swelling, which may be present for years. There are cases with bilateral synchronous or metachronous involvement. There are reported cases of spermatocytic seminoma with metastases. However, only one well-documented case is known. Spermatocytic seminoma is rarely associated with sarcoma; these tumors metastasize as sarcomas.
11. A 30-year-old man presented with a cystic mass in the head of the right epididymis (Fig. 11.3). The most likely diagnosis is:
a. Papillary cystadenoma
b. Simple epididymal cyst
c. Appendix epididymis
d. Paradidymis
e. Benign papillary mesothelioma
View Answer
11. a. Papillary cystadenoma of epididymis is a benign tumor that accounts for about one third of all primary epididymal tumors. Mean age is 36 years. It often involves the head of the epididymis. About two thirds of papillary cystadenomas of the epididymis occur in patients with von Hippel-Lindau syndrome. In this setting, they are more frequently bilateral. The tumor consists of cuboidal to low columnar clear cells lining dilated ducts and papillae with a single- or a doublelayer epithelium. The tumors resemble clear cell renal cell carcinoma.
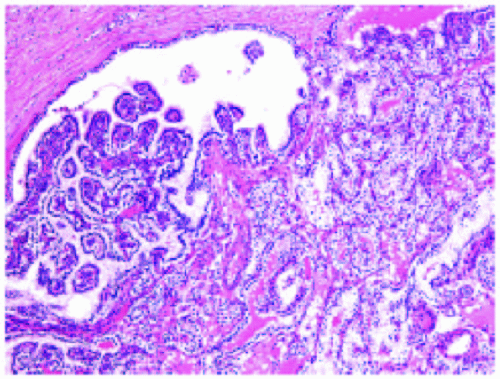 Figure 11.3 |
12. A 35-year-old man was found to have a left testicular mass. On gross examination, the lesion consisted of a small (around 10 mm) whitish encapsulated nodule located in the testicular parenchyma (Fig. 11.4). The diagnosis is:
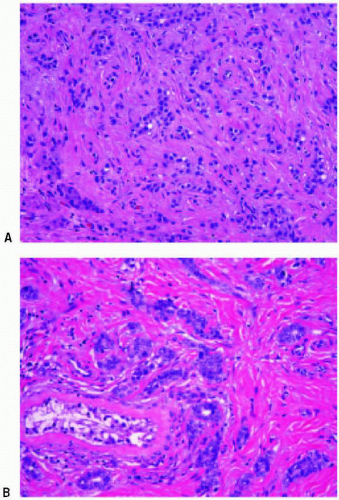 Figure 11.4 |
a. Adenomatoid tumor
b. Metastatic carcinoma of the prostate
c. Sclerosing Sertoli cell tumor
d. Metastatic carcinoma of the lung
e. Benign papillary mesothelioma
View Answer
12. c. Sertoli cell tumors account for about 1% of all primary testicular tumors. They can occur at any age but are most common in the fourth to fifth decades (it ranges from 20-80 years old). There are several subtypes: Sertoli cell tumors not otherwise specified, largecell calcifying Sertoli cell tumor, sclerosing Sertoli cell tumor, lipid-rich Sertoli cell tumor, and the Sertoli cell tumor with heterologous elements. Sclerosing Sertoli cell tumors are not associated with hormonal symptoms. Grossly, the lesion is usually small (0.4-1.5 cm in diameter) and consists of solid, white to yellow-tan nodules. Microscopically, it is composed of cords, solid or hollow tubules, and nests of Sertoli cells set in a densely collagenous stroma. The nuclei vary from large to small, and the cytoplasm is pale and sometimes vacuolated. Immunohistochemically, vimentin and inhibin are present in the neoplastic cells. Pancytokeratin (AE1/3) may be focally positive. All the reported cases had a benign outcome.
13. A 46-year-old man presented with a firm spermatic cord mass of several years’ duration. It has increased in size over the past 2 to 3 years. The tumor was excised along with a hydrocele sac (Fig. 11.5). The most likely diagnosis is:
a. Malignant mesothelioma
b. Sclerosing liposarcoma
c. Nodular periorchitis
d. Vasitis nodosa
e. Benign papillary mesothelioma
View Answer
13. c. Nodular periorchitis (fibrous pseudotumor, fibromatous periorchitis) of the tunica and paratesticular soft tissue typically arise as painless scrotal masses that may be associated with a hydrocele or history of trauma or infection. Typically, these masses are multinodular, but in rare cases they are diffuse, encasing the testis. Microscopically, they consist of collagen with calcifications and focal inflammatory cells.
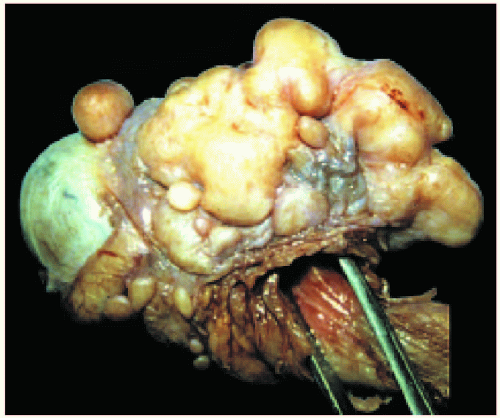 Figure 11.5 |
14. A 46-year-old man presented with a heavy feeling, pain, and swelling in the scrotum (Fig. 11.6). HCG was slightly elevated. AFP was negative. The diagnosis is:
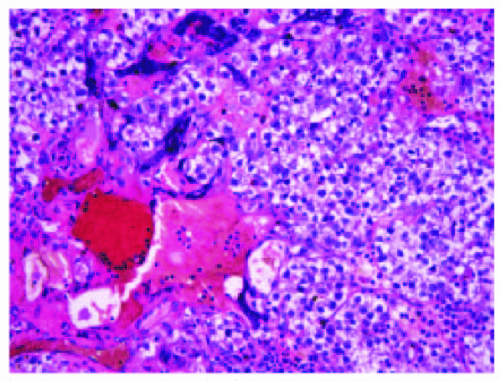 Figure 11.6 |
a. Seminoma with syncytiotrophoblastic cells
b. Seminoma
c. Embryonal carcinoma
d. Choriocarcinoma
e. Spermatocytic seminoma
View Answer
14. a. This is a typical seminoma associated with varying numbers of large multinucleated giant cells with abundant pink cytoplasm. Often, the cytoplasm contains vacuoles, which may contain erythrocytes. The syncytiotrophoblastic cells are usually accompanied by hemorrhage. They can cause elevated serum levels of HCG depending on their number. This type of seminoma has the same prognosis as pure seminoma.
15. A mother detected an enlarged testis in her 2-year-old boy. The orchiectomy specimen revealed a circumscribed tumor with multiple small cysts replacing most of the testis (Fig. 11.7). Some of the cysts contained mucoid fluid. What is the diagnosis?
a. Yolk sac tumor
b. Embryonal carcinoma
c. Mixed germ cell tumor
d. Teratoma
e. Cystic dysgenesis
View Answer
15. d. Teratomas are often cystic and consist of all three germinal layers (ectoderm, mesoderm and endoderm). The cysts are lined by various types of epithelium. Some are squamous with keratin-filled lumina, others are mucinous and resemble large bowel epithelium, or respiratory in type (pseudostratified and ciliated). Between the cysts are hair follicles, sweat and sebaceous glands, smooth muscle, and fat. All the tissues may be mature, immature, or both. Teratoma in the prepubertal child is diploid and benign. However, in the postpubertal male, teratomas (mature or immature) are commonly aneuploid and present with metastasis in about 30% to 40% at initial presentation. Therefore, teratomas in the adult male are not referred to as benign irrespective of their histologic appearance.
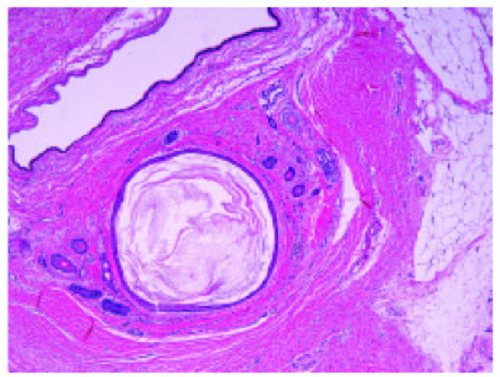 Figure 11.7 |
16. A 21-year-old man noticed a right testicular mass of 1 month’s duration. In the lower pole of the testis was a mass measuring 5 cm in diameter. Grossly, it had a variegated appearance. The histology (Fig. 11.8A and 11.8B) is typical of:
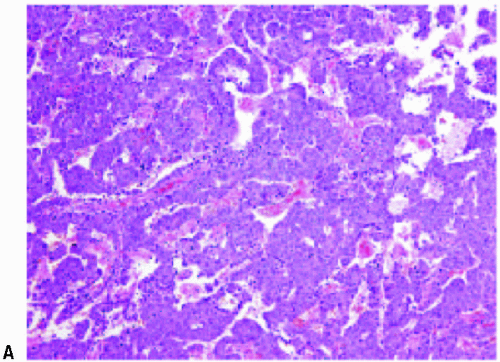 Figure 11.8 (continues) |
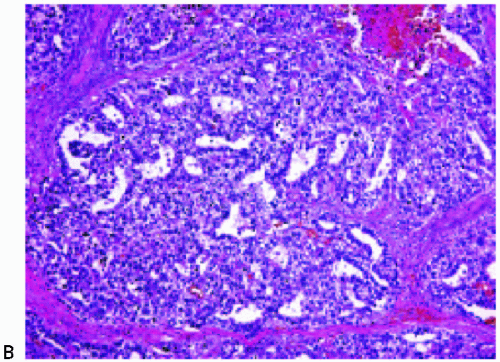 Figure 11.8 (continues) |
a. Embryonal carcinoma and seminoma
b. Embryonal carcinoma and yolk sac tumor
c. Solid yolk sac tumor
d. Embryonal carcinoma
e. Malignant Sertoli cell tumor
View Answer
16. d. Although some areas consist of solid sheets of cells, much of the tumor is arranged in glandular and papillary structures. The cells are large and the nuclei tend to be irregular and variable in shape or contour. The cells of embryonal carcinoma differ from those of seminoma, chiefly in that cell borders are usually ill-defined, nuclei are vacuolated rather than stippled with fine chromatin granules, and the nuclei tend to be more irregular in shape compared with the rounded seminoma cell. The cells are larger than those of seminoma.
17. A 24-year-old man with an infertility problem had a testicular biopsy (Fig. 11.9A and 11.9B). The histology indicates:
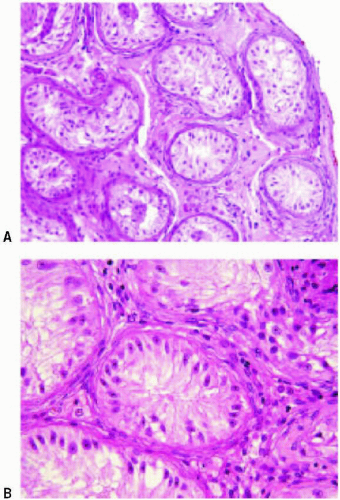 Figure 11.9 |
a. Sertoli-cell-only syndrome
b. Healed mumps orchitis
c. Klinefelter syndrome
d. Intratubular malignant germ cell neoplasia unclassified
e. Maturation arrest
View Answer
17. a. In Sertoli cell-only syndrome, seminiferous tubules are devoid of germ cells and are lined by thin palestaining Sertoli cells only (wind-swept appearance).
18. A 68-year-old man complained of gradually enlarging testis of 6 months’ duration. No tumor markers were performed. The prostate was also hard. The testis measured 6 × 5 × 4 cm and contained a homogeneous yellowish white tumor that had some nodularity, replaced the parenchyma, and extended into the epididymis (Fig. 11.10). What is the correct diagnosis?
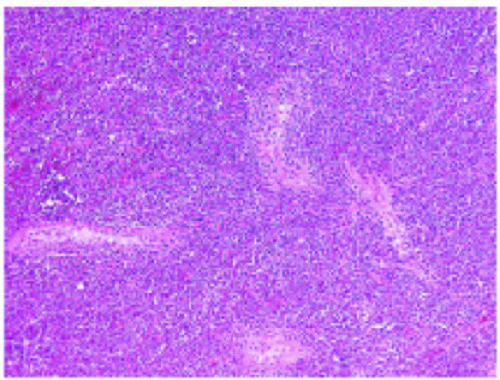 Figure 11.10 |
a. Seminoma
b. Lymphoma
c. Leydig cell tumor
d. Metastatic lung carcinoma
e. Spermatocytic seminoma
View Answer
18. b. The tumor is located mainly in the interstitium. Note that the cells have very little cytoplasm in contrast to seminoma. The nuclei are irregular in shape and smaller than seminoma cells. The prostate biopsy also revealed lymphoma. Lymphomas of the testis may be the primary manifestation of this disease and are usually seen in men older than 50 years of age. Generalized lymphoma usually develops within 2 years, and bilateral testicular involvement is seen in about 25% of cases.
19. A 67-year-old man had swelling of the left scrotum for 3 weeks, which initially was thought to be a
hydrocele. When herniorrhaphy was performed, the spermatic cord was found to be enlarged (7-8 cm in diameter). A tumor appeared to arise near the epididymis and extend up the cord. The tunica was studded with numerous granular, nodular lesions. The testicular parenchyma was grossly uninvolved (Fig. 11.11). The diagnosis is:
hydrocele. When herniorrhaphy was performed, the spermatic cord was found to be enlarged (7-8 cm in diameter). A tumor appeared to arise near the epididymis and extend up the cord. The tunica was studded with numerous granular, nodular lesions. The testicular parenchyma was grossly uninvolved (Fig. 11.11). The diagnosis is:
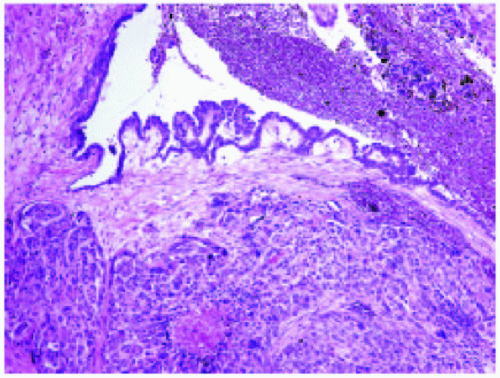 Figure 11.11 |
a. Malignant mesothelioma
b. Adenomatoid tumor
c. Metastatic carcinoma of the prostate
d. Yolk sac tumor
e. Reactive mesothelial proliferation
View Answer
19. a.Macroscopically, the tumors consist of nodular excrescences studying the tunica with or without diffuse thickening of the tunica vaginalis and/or albuginea. Histologically, the mesothelial lining of the tunica is prominent and multilayered. The cells extend into the adjacent soft tissue as an epithelial-like tumor with solid areas, as well as tubules, acinar, and papillary structures. The cells generally contain abundant pink cytoplasm with nuclear pleomorphism. The lining mesothelial cells of the tunica are hyperchromatic, hyperplastic, and represent the site of origin of the neoplasm. Four months following surgery, tumor nodules recurred in the cord adjacent to the incision. Malignant mesothelioma of the tunica is often a manifestation of systemic disease involving peritoneal and/or pleural surfaces.
20. A mother noticed that her child had an enlarged right testis (Fig. 11.12A and 11.12B). What is the diagnosis?
a. Mature teratoma
b. Gonadoblastoma
c. Sertoli cell tumor
d. Yolk sac tumor
e. Adenomatoid tumor
View Answer
20. a.Microscopically, yolk sac tumors are variable and 10 subtypes are recognized. In most instances, several of these coexist. The glandular/alveolar pattern, microcystic, and micropapillary patterns are the most common. The neoplasm forms numerous glandular spaces, some of which are quite large, others minute. Some of the smaller glands resemble fat cells or endothelial-lined spaces, but these, in fact, are lined by flattened or cuboidal cells with clear or pink cytoplasm and irregular vesicular nuclei. There is also a papillary component. Some of these have a prominent central vascular core constituting the so-called glomeruloid structure referred to as the Schiller-Duval body (Fig. 11.12A).
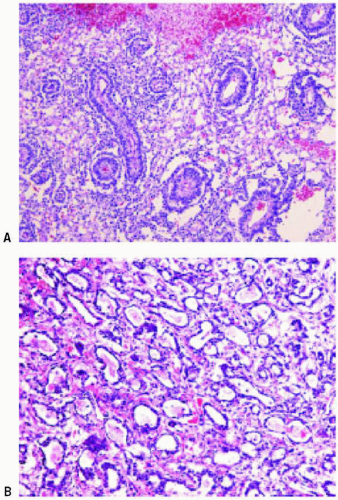 Figure 11.12 |
21. A 27-year-old man presented with a palpable groin mass (Fig. 11.13). He had no detectable testis in the scrotum. What is the diagnosis?
a. Mixed germ cell tumor
b. Seminoma
c. Undescended testis
d. Embryonal carcinoma
e. Intratubular germ cell neoplasia unclassified
View Answer
21. c. In cryptorchid testis, the walls of the tubules have a hyalinized, thickened appearance. The tubules contain only Sertoli cells, recognized by their stringy, vacuolated cytoplasm and the fact that their nuclei have prominent nucleoli. The best evidence of cryptorchidism is the presence of small, tightly packed seminiferous tubules filled with immature Sertoli cells. In contrast to the Sertoli cells in the adjacent atrophic tubules, the immature Sertoli cells appear very dark with elongated hyperchromatic nuclei.
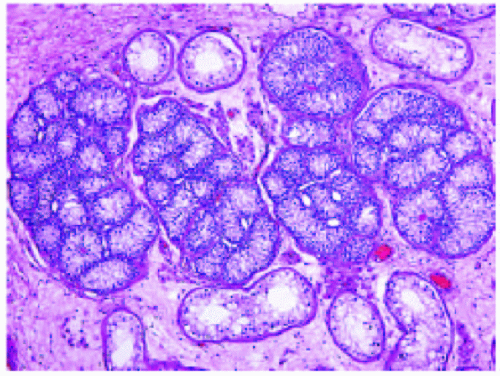 Figure 11.13 |
22. This 23-year-old man had a testicular biopsy (Fig. 11.14). Which condition does he have?
a. Leydig cell tumor
b. Seminoma
c. Cryptorchid
d. Leydig cell hyperplasia
e. Sertoli cell tumor
View Answer
22. d. The section shows a large nodule of Leydig cells. It contains seminiferous tubules. The chief difference between Leydig cell hyperplasia and Leydig cell tumor is the presence of entrapped tubules seen in hyperplasia. The reason for the Leydig cell hyperplasia is not apparent.
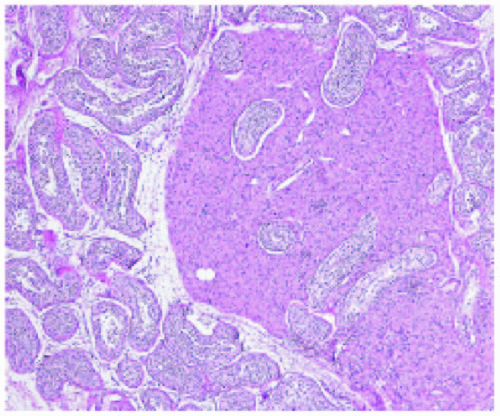 Figure 11.14 |
23. A 27-year-old man presented with an asymptomatic right scrotal mass discovered during a routine physical
examination. The cut surface of the testis revealed a well demarcated, whitish-gray round cyst. It was 1.7 cm in diameter with a laminated, soft, friable center (Fig. 11.15). The testis was otherwise normal. The diagno sis is:
examination. The cut surface of the testis revealed a well demarcated, whitish-gray round cyst. It was 1.7 cm in diameter with a laminated, soft, friable center (Fig. 11.15). The testis was otherwise normal. The diagno sis is:
a. Seminoma
b. Spermatocele
c. Leydig cell tumor
d. Epidermoid cyst
e. Dermoid cyst
View Answer
23. d. The section shows the wall of a cyst composed of mature squamous epithelium, consistent with epidermoid cyst. The cyst contains keratin. The absence of skin appendages distinguishes this cyst from the dermoid cyst. This lesion is benign. The question if this tumor is a monophasic teratoma is still unsettled. Rare epidermoid cysts are associated with intratubular germ cell neoplasia, unclassified.
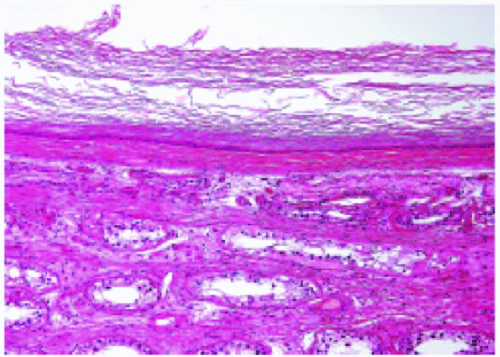 Figure 11.15 |



