Loin Pain Hematuria Syndrome
Xin Gu, MD
Key Facts
Etiology/Pathogenesis
Unknown or tubular obstruction from intranephron hemorrhage
Clinical Issues
LPHS is a diagnosis of exclusion
Microscopic Pathology
Normal or nonspecific
Arteriolar sclerosis and isolated glomerulosclerosis
Focal interstitial fibrosis or edema
RBCs and RBC casts in tubules
Immunofluorescence
Mesangial IgM/C3 reaction, arteriolar C3
Electron microscopy
Segmental thinning of GBM
Top Differential Diagnoses
Urologic causes
Neoplasms
Occult renal lithiasis
Kidney or bladder infection
Cystic renal disease
Glomerular diseases
IgA nephropathy
Thin basement membrane nephropathy
Glomerular diseases with nephritic presentation
Renal vascular diseases
Isolated polyarteritis nodosa
Vascular malformations
Diagnostic Checklist
Biopsy important to exclude specific causes
 In general, kidney biopsies from LPHS patients do not reveal specific pathology. This image shows a normal glomerulus with patent capillary loops and delicate walls. The mesangium is inconspicuous. |
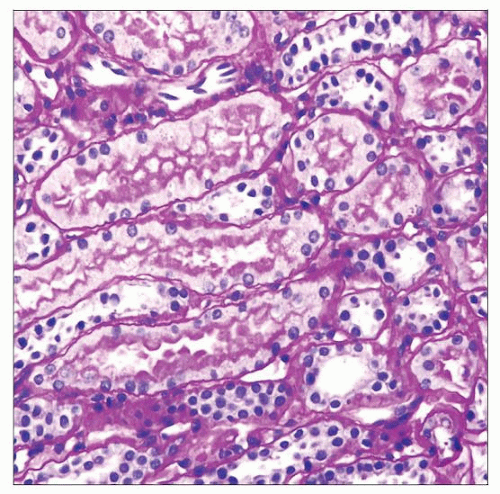 This biopsy from an LPHS patient shows a histologically normal cortical tubulointerstitium. The proximal tubules show preserved brush borders. The tubules are back-to-back, and the interstitium is inconspicuous. |
TERMINOLOGY
Abbreviations
Loin pain hematuria syndrome (LPHS)
Definitions
Recurrent pain in lower flanks and intermittent hematuria without identifiable cause
ETIOLOGY/PATHOGENESIS
Unclear
Proposed classification: Idiopathic disease vs. clinical mimics
LPHS: Idiopathic disease
Possible etiology: Glomerular capillary hemorrhage
RBC and RBC casts obstruct tubules, leading to backleak of glomerular filtration
Tubular injury and interstitial edema lead to capsular distension and pain
Clinical mimics of LPHS
IgA nephropathy
Thin basement membrane nephropathy
Occult nephrolithiasis
Vascular malformation
Inflammatory renal vascular diseases
Vascular spasm
CLINICAL ISSUES
Epidemiology
Incidence
Diagnosis of exclusion, so incidence cannot be estimated from population-based studies
Age
Children and adults from 1st to 6th decade
Median age: Mid 30s
Gender
More common in females (70%) than in males (30%)
Presentation
Severe recurrent lower flank pain and hematuria
Pain is unilateral at initial presentation
Radiates to abdomen, inguinal and inner thigh
Eventually may develop bilateral flank pain
Hematuria may be gross or microscopic
Pain may not always be associated with hematuria
Physical examination is unremarkable and nonspecific
Costovertebral angle tenderness
Low-grade fever may be present
No hypertension, except preexisting
Laboratory Tests
Urine analysis may show RBCs and RBC casts
Treatment
Options, risks, complications
Multidisciplinary pain management
Analgesia: NSAIDs and opioids
Intraureteric capsaicin
Nerve blockade
Antidepressants
Nephrectomy with autotransplantation
Prognosis
Long-term prognosis is excellent
Renal function is well preserved
Spontaneous resolution in 30% after conservative treatment
IMAGE FINDINGS
Radiographic Findings
Normal or nonspecific
Minor vascular alterations may present
MICROSCOPIC PATHOLOGY
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


