Ligation, Stripping, and Harvesting of the Saphenous Vein
Amir F. Sleiman
Jamal J. Hoballah
This chapter first covers excision of the greater and lesser saphenous veins for management of varicosities, and then harvesting for use as a vascular conduit.
Superficial venous insufficiency and varicose vein formation can develop in the trunk of the greater or lesser saphenous veins and their respective branches. The resulting varicose veins may be asymptomatic or cause a variety of symptoms, including heaviness in the leg, itching or burning sensation, and venous stasis ulcerations. Compression stockings are often used as the first line of therapy, but symptoms may persist. Difficulties with compliance, particularly during hot weather, and dissatisfaction with the cosmetic appearance of the legs cause many patients to seek other therapy. Surgical removal, described here, has stood the test of time as an effective management. The key principle remains to remove all varicose veins using the smallest skin incisions possible and to minimize complications. Endovascular ablation using radiofrequency or laser catheters have gained popularity as a less invasive treatment option. The procedure can be performed in the office under local tumescent anesthesia with mild sedation. Nevertheless, many patients may opt for the surgical removal especially when the saphenous vein is very dilated or very superficial.
The saphenous vein is usually stripped by inserting a stripper from one end of the vein toward the other. The stripper is usually passed from the distal end toward the groin to avoid catching on valve cusps. The distal end of the vein is then ligated around the stripper, divided, and then pulled out. The branch veins are usually excised using very small incisions through which the branch may be grasped and avulsed—the so-called “stab incision and vein avulsion or stab phlebectomy” technique. Traditionally, the greater saphenous vein was stripped from the ankle to the groin. However, this approach was found to be associated with saphenous nerve injury, resulting in loss of cutaneous sensation in the medial leg and ankle, because of proximity and adherence of the saphenous nerve to the greater saphenous vein in the lower leg. In addition, the posterior arch vein is usually the main pathway of incompetence in the leg rather than the saphenous vein. Consequently, it is recommended to strip the greater saphenous vein from just below the knee level to the groin. The lowest recurrence rates in the surgical options are obtained by combining stripping of the saphenous vein with excision of the associated branches.
Frequently, varicosities are limited to these branches, and the main trunks are relatively normal and of small caliber. Stripping the trunk in this situation may deprive the patient of a vein that could be a useful conduit in the future, should the need for lower extremity or coronary revascularization arise. Thus, some surgeons recommend avoiding stripping the saphenous veins when the varicosities are limited to the branches and the duplex ultrasound shows no evidence of significant reflux in the greater saphenous vein. In this situation, only stab avulsion of the varicosities is performed. This procedure may be complemented by ligation and division of the saphenofemoral junction if this is proved incompetent by duplex ultrasound evaluation.
SCORE™, the Surgical Council on Resident Education, classified operation for varicose veins as an “ESSENTIAL COMMON” procedure.
STEPS IN PROCEDURE
Stripping Greater Saphenous Vein
A 3- to 4-cm transverse incision in the inguinal crease centered 1 cm medial to the femoral pulse
If preoperative vein mapping was performed, center incision over vein
Skeletonize saphenofemoral junction
Ligate and divide all veins draining into it
Ligate and divide the greater saphenous vein 2 cm distal to saphenofemoral junction
Suture-ligate the saphenofemoral junction with 2-0 silk
Make 1-cm incision over marked greater saphenous vein few centimeters below the knee
Ligate distal end of vein
Introduce stripper, guide it to the groin, and allow it to exit the ligated end of the vein
Apply olive-shaped head to distal end of stripper and secure with tie
Pull the stripper to extract vein and stripper from groin incision
If you plan it to strip to ankle, make small incision 1 cm anterior and superior to medial malleolus
Identify and preserve the saphenous nerve
Pass stripper and remove vein as previously described
Irrigate wounds and close
Apply compressive dressing
Stab Avulsion of Branch Varicosities
Mark all branches with patient standing upright
A 2- to 3-mm stab incision along side of branch
Introduce crochet hook and hook up the vein
Clamp segment of vein and divide it
Avulse as much of each segment of vein as possible
Harvesting Greater Saphenous Vein for Reverse or Nonreverse Bypass Procedures
Small incisions over vein (preoperative vein marking helps)
Alternatively, harvest endoscopically
Carefully ligate all branches flush with vein
Gently flush with chilled whole blood, cold Ringer’s lactate, or other solution
Avoid overdistension by monitoring pressure
HALLMARK ANATOMIC COMPLICATIONS
Injury to saphenous nerve
Injury to femoral vein
Recurrence of varicosities
LIST OF STRUCTURES
Femoral artery
Common femoral vein
Greater (great) saphenous vein; saphenofemoral junction
Lesser saphenous vein
Femoral Nerve
Saphenous nerve
Medial femoral cutaneous nerve
Posterior femoral cutaneous nerve
Sural nerve
Lateral cutaneous nerve
Musculocutaneous nerve
Patella
Lateral malleolus
Medial malleolus
Inguinal crease
Pubic tubercle
Fascia Lata
Saphenous hiatus (fossa ovalis)
Adductor canal
Sartorius muscle
Gastrocnemius muscle
Stripping the Greater Saphenous Vein: Exposure of the Saphenofemoral Junction (Fig. 130.1)
Technical Points
A 3- to 4-cm transverse incision in the inguinal crease has an excellent cosmetic result. Preoperative duplex ultrasonography allows precise mapping of the veins, including the saphenofemoral junction. It can be especially helpful in determining the location of the greater saphenous vein just below the knee when the leg is large or the patient is overweight. If preoperative mapping was performed, center the skin incision over the saphenofemoral junction. Alternatively, use anatomic landmarks and begin the inguinal crease incision 1 cm medial to the femoral pulse and extend it medially for 3 to 4 cm (Fig. 130.1A). If the femoral pulse is not palpable, identify a point midway between the pubic tubercle and the anterosuperior iliac spine and begin the skin incision 1 cm medial to this point. Deepen the incision through the subcutaneous tissues and Scarpa fascia to expose the vein. Often, one of the branches draining into the saphenofemoral junction is encountered first; trace
this branch to the saphenofemoral junction. Skeletonize the saphenofemoral junction, and ligate and divide all the branches draining into it. These branches include the epigastric vein, the circumflex iliac vein, the external pudendal vein, and the anterolateral vein.
this branch to the saphenofemoral junction. Skeletonize the saphenofemoral junction, and ligate and divide all the branches draining into it. These branches include the epigastric vein, the circumflex iliac vein, the external pudendal vein, and the anterolateral vein.
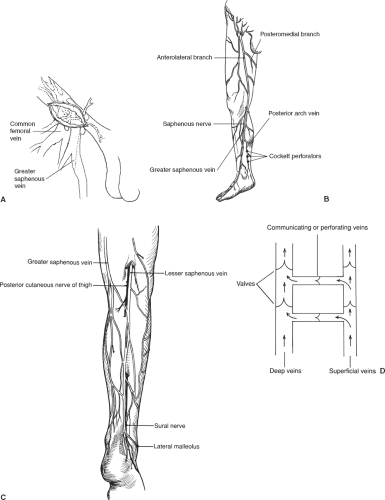 Figure 130.1 Stripping the greater saphenous vein: Exposure of the saphenofemoral junction. A: Anatomy of groin. B: Greater saphenous vein. C: Lesser saphenous vein. D: Arrangement of valves in deep and superficial systems and role of perforating veins. |
Ligate the greater saphenous vein 2 cm distal to the saphenofemoral junction. Apply a clamp to the saphenofemoral junction and divide the saphenous vein, suture-ligating the saphenofemoral junction with 2-0 silk.
Anatomic Points
The greater saphenous vein originates on the medial side of the arch of the dorsum of the foot (Fig. 130.1B). It ascends anterior to the tip of the medial malleolus and then over the subcutaneous surface of the lower end of the tibia. The greater saphenous vein continues up to the knee, where it moves posterior to the back part of the internal condyle of the femur and then follows the course of the sartorius muscle up to the inguinal region. Below the knee, the greater saphenous vein lies in a superficial subcutaneous plane and is accompanied by the great saphenous nerve. The saphenous nerve is a branch of the femoral nerve transmitting sensation from the medial aspect of the leg and foot. Above the knee, the greater saphenous vein gradually moves into a deeper subcutaneous plane and penetrates the fascia lata in the upper thigh through the fossa ovalis to join the common femoral vein. In the thigh, the greater saphenous vein is accompanied by branches of the medial femoral cutaneous nerve. The length of the greater saphenous vein in an adult male is estimated to be 60 cm. Frequently, a duplicate system can be found in the thigh (35%) or in the leg. The vein contains approximately 8 to 12 valves, with more valves present in the below-knee segment.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


