Large Cell Lymphoma
Scott R. Owens, MD
Key Facts
Terminology
“Large”: Cells with nucleus ≥ macrophage nucleus or > 2x normal lymphocyte nucleus
Etiology/Pathogenesis
Secondary DLBCL arises from preexisting low-grade lymphoma (“progression” or “transformation”)
Some secondary DLBCL may “overgrow” underlying low-grade component, obscuring evidence of transformation
DLBCL arises in settings positive for Epstein-Barr Virus (EBV) more often than cases arising sporadically
Clinical Issues
GI tract most common extranodal site of DLBCL
May be seen in association with underlying MALT lymphoma, suggesting transformation
Blood and bone marrow involvement uncommon at presentation
May be curable with appropriate therapy
Microscopic Pathology
Diffuse replacement of underlying tissue architecture
Discohesive, large cells
3 recognized variants
Centroblastic is most common variant
Immunoblastic
Anaplastic
Diagnostic Checklist
Estimation of cell size aided by comparison to nearby cells
Discohesive nature of lymphoma cells helpful in differentiation from carcinoma
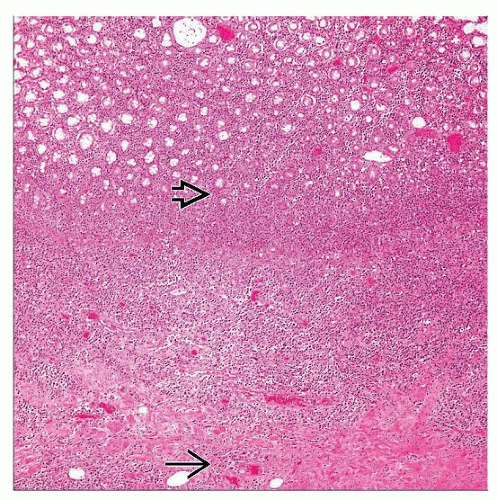 Hematoxylin & eosin shows intestinal diffuse large B-cell lymphoma infiltrating and disrupting the muscularis propria  and extending into the mucosa and extending into the mucosa  . . |
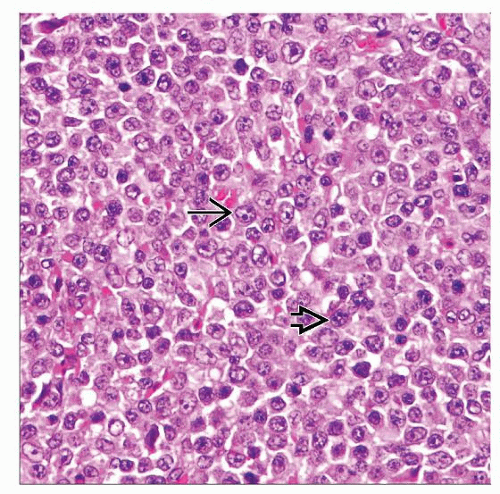 Hematoxylin & eosin shows a high-power view of DLBCL. Some cells have 1 prominent nucleolus (immunoblast-like)  , and others have multiple inconspicuous nucleoli (centroblast-like) , and others have multiple inconspicuous nucleoli (centroblast-like)  . . |
TERMINOLOGY
Abbreviations
Large cell lymphoma (LCL)
Synonyms
Diffuse large B-cell lymphoma (DLBCL)
Definitions
Neoplasm composed of large B lymphocytes diffusely infiltrating tissue
“Large”: Cells with nucleus ≥ macrophage nucleus or > 2x normal lymphocyte nucleus
ETIOLOGY/PATHOGENESIS
Primary
Arises de novo
No known etiology for most cases
Secondary
Arises from preexisting low-grade lymphoma (“progression” or “transformation”)
Mucosa-associated lymphoid tissue (MALT) lymphoma
Follicular lymphoma (FL)
Chronic lymphocytic leukemia (CLL), small lymphocytic lymphoma (SLL)
Some secondary DLBCL may “overgrow” underlying low-grade component, obscuring evidence of transformation
Immunodeficiency
Significant risk factor
DLBCL arises in settings positive for Epstein-Barr virus (EBV) more often than cases arising sporadically
CLINICAL ISSUES
Epidemiology
Incidence
30-40% of all adults with non-Hodgkin lymphoma (NHL)
Age
Most common in older patients (median 7th decade)
Also occurs in young patients
Gender
Affects males slightly more often than females
Site
≥ 40% of cases extranodal at presentation
GI tract most common extranodal site of DLBCL
DLBCL most common lymphoma of GI tract
Stomach
May be seen in association with underlying MALT lymphoma, suggesting transformation
Small &/or large intestine
May be seen as progression/transformation of follicular lymphoma or MALT lymphoma
Regional lymph nodes
May be involved by DLBCL &/or underlying lower grade lymphoma
Presentation
May be asymptomatic
Abdominal pain
Deep mass
Ulcer
Endoscopic Findings
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


