Large Cell (Anaplastic) Carcinoma
Key Facts
Clinical Issues
Cough
Chest pain
Dyspnea
Generally poor prognosis with short survival
Most commonly seen in smokers
Image Findings
Periphery of lungs
Generally large (> 5 cm in greatest diameter)
Microscopic Pathology
Neoplastic population is composed of large tumor cells without histologic evidence of glandular or squamous differentiation
Variegated histology with different growth patterns, including
Large cell carcinoma, NOS
Giant cell carcinoma
Clear cell carcinoma
Large cell carcinoma with “rhabdoid” features
Tumor cells are usually very large and measure 3-4x the size of a normal histiocyte
Nuclei are enlarged and may be multilobated or multinucleated
Frequent mitotic figures with abnormal mitoses
Lymphoid cell emperipolesis
Syncytiotrophoblastic-like tumor cells
Ancillary Tests
Most cases are positive for broad-spectrum keratin and low-molecular weight cytokeratins (CAM5.2)
Tumor cells are negative for neuroendocrine markers (chromogranin, synaptophysin, CD56)
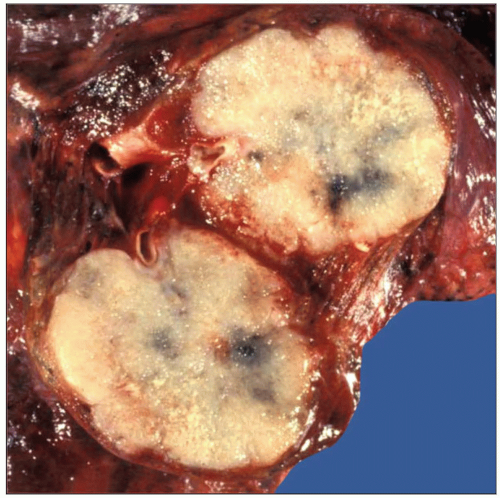 Cut surface shows gross appearance of large cell (anaplastic) carcinoma of the lung characterized by a large, well-circumscribed, tan-cream tumor with foci of hemorrhage and necrosis. |
 Histologic appearance of large cell (anaplastic) carcinoma of the lung shows sheets of large tumor cells without evidence of glandular or squamous differentiation. |
TERMINOLOGY
Synonyms
Pleomorphic carcinoma, giant cell carcinoma, rhabdoid carcinoma, large cell undifferentiated carcinoma
Definitions
Malignant epithelial neoplasm of the lung displaying large cell or anaplastic morphology with no specific histologic features of differentiation
ETIOLOGY/PATHOGENESIS
Etiology
Originates from a putative primitive progenitor cell capable of multidirectional differentiation
CLINICAL ISSUES
Epidemiology
Incidence
Accounts for approximately 8-10% of all lung cancers
Most commonly seen in smokers
Age
Adults from 50-70 years old (average: 60 years)
Gender
Male predilection
Presentation
Cough
Chest pain
Dyspnea
Treatment
Surgical approaches
Surgical excision is recommended for stage I tumors
Adjuvant therapy
Adjuvant chemotherapy is indicated for stage II tumors
Radiation
Radiotherapy has also been employed in stage I and II tumors
Combination chemotherapy combined with radiation is employed for stage III tumors
Prognosis
Generally poor prognosis with short survival
IMAGE FINDINGS
General Features
Location
Periphery of lungs
Size
Generally large (> 5 cm in greatest diameter)
Morphology
Subpleural mass with invasion of pleura, chest wall, or adjacent structures
MACROSCOPIC FEATURES
General Features
Large, well-circumscribed tumor mass with soft, tan-white tissue that bulges above cut surface
Frequent areas of hemorrhage and necrosis
MICROSCOPIC PATHOLOGY
Histologic Features
Neoplastic population is composed of large tumor cells without histologic evidence of glandular or squamous differentiation
Variegated histology with different growth patterns
Large cell carcinoma, NOS
Sheets of large tumor cells with vesicular chromatin, prominent nucleoli, and abundant rim of cytoplasm
May display discohesive growth pattern that resembles a sarcoma (e.g., malignant fibrous histiocytoma, pleomorphic subtype)
May be accompanied by abundant inflammatory cell infiltrate in the stroma admixed with tumor cells (“inflammatory” subtype)
May display prominent engulfment of lymphoid cells (emperipolesis) by tumor cells
Giant cell carcinoma
Sheets of large, pleomorphic tumor cells that are often multilobated and display prominent multinucleation
Tumor cells may resemble syncytiotrophoblastic tumor cells of choriocarcinoma
Pleomorphic tumor cells may secrete β-HCG
Clear cell carcinoma
Tumor composed of sheets of large tumor cells with abundant clear cytoplasm
No histologic evidence of glandular or squamous differentiation
May show abortive features of glandular or squamous differentiation ultrastructurally
Large cell carcinoma with “rhabdoid” features
Sheets of large, atypical tumor cells displaying large eosinophilic cytoplasmic inclusions
Eosinophilic inclusions may displace nucleus to periphery of cell
Eosinophilic inclusions contain admixture of cytokeratin and vimentin intermediate filaments
Cytologic Features
Tumor cells are usually very large and measure 2-4x the size of a normal histiocyte
Nuclei are enlarged and may be multilobated or multinucleated
Frequent mitotic figures with abnormal mitoses
Tumor cell emperipolesis
Syncytiotrophoblastic-like tumor cells
ANCILLARY TESTS
Immunohistochemistry
Most cases are positive for broad-spectrum keratin and low-molecular weight cytokeratins (CAM5.2)
Tumor cells are negative for neuroendocrine markers (chromogranin, synaptophysin, CD56)
Pleomorphic tumor cells may be positive for β-HCG
DIFFERENTIAL DIAGNOSIS
Pleomorphic High-Grade Sarcoma (MFH)
Discohesive population of pleomorphic tumor cells
Strong vimentin positivity; absence of reactivity for epithelial markers
Rare cases of MFH may show focally aberrant expression of cytokeratin
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


