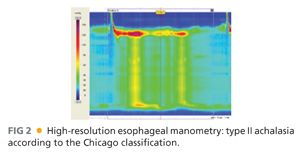
■ Esophageal manometry is the gold standard for the diagnosis of achalasia. Lack of peristalsis and absent or incomplete LES relaxation in response to swallowing are the key criteria for the diagnosis. The LES is hypertensive in only about 50% of patients.3 Recently, a new classification of esophageal achalasia has been proposed based on high-resolution manometry (HRM): type I, classic, with minimal esophageal pressurization; type II, achalasia with panesophageal pressurization; and type III, achalasia with spasm (FIG 2).4
■ Ambulatory pH monitoring is important in untreated patients when the diagnosis is uncertain in order to distinguish between GERD and achalasia. Postoperatively, ambulatory pH monitoring can be performed to rule out GER that is present in about 30% to 40% of cases after Heller myotomy and is often asymptomatic.5
SURGICAL MANAGEMENT
Preoperative Planning
■ A careful systematic evaluation and the tests described before should be performed in every patient before treatment.
Positioning
■ After induction of general endotracheal anesthesia, the patient is positioned supine in low lithotomy position with the lower extremities extended on stirrups, with knees flexed 20 to 30 degrees or straight if using a split-leg table.
■ To avoid sliding as a consequence of the steep reverse Trendelenburg position used during the procedure, a beanbag is inflated to create a “saddle” under the perineum.
■ Because increased abdominal pressure from pneumoperitoneum and the steep reverse Trendelenburg position decrease venous return, pneumatic compression stockings are always used as prophylaxis against deep venous thrombosis.
■ An orogastric tube is placed to keep the stomach decompressed during the procedure and it is removed before starting the myotomy.
■ A Foley catheter is inserted at the beginning of the operation and removed at the end.
■ The surgeon stands between the patient’s legs. The first and second assistants stand on the right and left side of the operating table (FIG 3).

TECHNIQUES
PLACEMENT OF PORTS
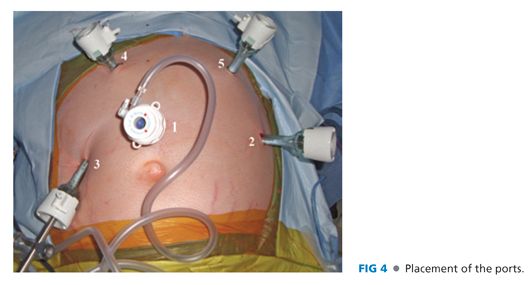
■ Five 10-mm trocars are used for the procedure (FIG 4).
■ The first incision is made in the midline 14 cm distal to the xiphoid process and a Veress needle is introduced into the peritoneal cavity. The peritoneal cavity is insufflated to a pressure of 15 mmHg. Subsequently, under direct vision, an optical port with a 0-degree scope (port 1) is placed. Once this port is placed, the 0-degree scope is replaced with a 30-degree scope and the other trocars are inserted under laparoscopic vision.
■ Port 2 is placed in the left midclavicular line at the same level of port 1. It is used by the assistant for traction on the gastroesophageal junction and as an instrument to take down the short gastric vessels.
■ Port 3 is placed in the right midclavicular line at the same level of the other two ports. A retractor is used through this port to lift the left lateral segment of the liver to expose the gastroesophageal junction. The retractor is held in place by a self-retaining system fixed to the operating table.
■ Ports 4 and 5 are placed under the right and left costal margins so that their axes and the camera form an angle of about 120 degrees. These ports are used by the operating surgeon.
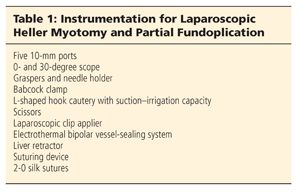
■ The instrumentation necessary for the laparoscopic myotomy is reported in Table 1.
DISSECTION
■ The gastrohepatic ligament is divided, beginning the dissection above the caudate lobe of the liver, where the ligament is thinner, and continuing toward the diaphragm until the right pillar of the crus is identified and separated from the esophagus by blunt dissection.
■ Subsequently, the peritoneum and the phrenoesophageal membrane overlying the esophagus are divided and the anterior vagus nerve is identified (FIG 5A).
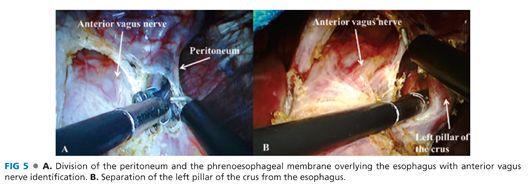
■ The left pillar of the crus is then separated from the esophagus (FIG 5B).
■ Blunt dissection is finally performed in the posterior mediastinum, laterally and anteriorly to the esophagus in order to have about 4 to 5 cm of esophagus without any tension below the diaphragm. Posterior dissection is necessary only if a partial posterior fundoplication is planned.
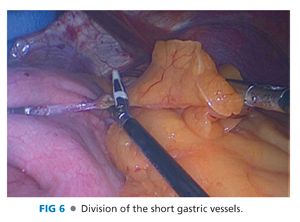
DIVISION OF THE SHORT GASTRIC VESSELS
■ The short gastric vessels are taken down all the way to the left pillar of the crus, starting from a point midway along the greater curvature of the stomach (FIG 6).6
MYOTOMY
■ The fat pad should be removed to expose the gastroesophageal junction after identification of the anterior vagus nerve.
■ Traction is then applied with a Babcock clamp, grasping below the gastroesophageal junction and pulling downward and to the left in order to expose the right side of the esophagus.
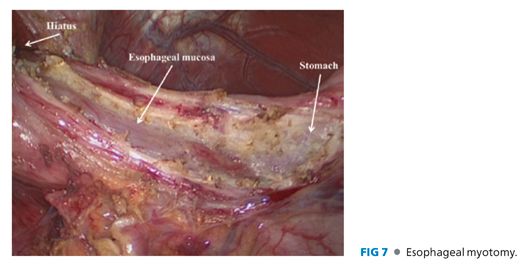
■ A myotomy is performed on the right side of the esophagus in the 11 o’clock position using a hook cautery. The proper submucosal plane is found using the cautery, about 3 cm above the gastroesophageal junction.
■ Once the mucosa is exposed, the myotomy is extended proximally for about 6 cm above the gastroesophageal junction and distally for 2.5 to 3 cm onto the gastric wall (FIG 7).7
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


