Although leg pain commonly signifies a musculoskeletal disorder, it can also result from a more serious vascular or neurologic disorder. The pain may arise suddenly or gradually and may be localized or affect the entire leg. Constant or intermittent, it may feel dull, burning, sharp, shooting, or tingling. Leg pain may affect locomotion, limiting weight bearing. Severe leg pain that follows cast application for a fracture may signal limb-threatening compartment syndrome. Sudden onset of severe leg pain in a patient with underlying vascular insufficiency may signal acute deterioration, possibly requiring an arterial graft or amputation. (See Highlighting causes of local leg pain.)
If the patient has acute leg pain and a history of trauma, quickly take his vital signs and determine the leg’s neurovascular status. Observe the patient’s leg position and check for swelling, gross deformities, or abnormal rotation. Also, be sure to check distal pulses and note skin color and temperature. A pale, cool, and pulseless leg may indicate impaired circulation, which may require emergency surgery.
HISTORY AND PHYSICAL EXAMINATION
If the patient’s condition permits, ask him when the pain began and have him describe its intensity, character, and pattern. Is the pain worse in the morning, at night, or with movement? If it doesn’t prevent him from walking, must he rely on a crutch or other assistive device? Also ask him about the presence of other signs and symptoms.
Find out if the patient has a history of leg injury or surgery and if he or a family member has a history of joint, vascular, or back problems. Also ask what medications he’s taking and whether they have helped to relieve his leg pain.
Begin the physical examination by watching the patient walk, if his condition permits. Observe how he holds his leg while standing and sitting. Palpate the legs, buttocks, and lower back to determine the extent of pain and tenderness. If a fracture has been ruled out, test the patient’s range of motion in the hip and knee. Also, check reflexes with the patient’s leg straightened and raised, noting any action that causes pain. Then compare both legs for symmetry, movement, and active range of motion. Additionally, assess sensation and strength. If the patient wears a leg cast, splint, or restrictive dressing, carefully check distal circulation, sensation, and mobility, and stretch his toes to elicit any associated pain.
MEDICAL CAUSES
♦ Bone cancer. Continuous deep or boring pain, commonly worse at night, may be the first symptom. Later, skin breakdown and impaired circulation may occur, along with cachexia, fever, and impaired mobility.
Highlighting causes of local leg pain
Various disorders cause hip, knee, ankle, or foot pain, which may radiate to surrounding tissues and be reported as leg pain. Local pain is commonly accompanied by tenderness, swelling, and deformity in the affected area.
Hip pain
Arthritis
Avascular necrosis
Bursitis
Dislocation
Fracture
Sepsis
Tumor
Knee pain
Arthritis
Bursitis
Chondromalacia
Contusion
Cruciate ligament injury
Dislocation
Fracture
Meniscal injury
Osteochondritis dissecans
Phlebitis
Popliteal cyst
Radiculopathy
Ruptured extensor mechanism
Sprain
Ankle pain
Achilles tendon contracture
Arthritis
Dislocation
Fracture
Sprain
Tenosynovitis
Foot pain
Arthritis
Bunion
Callus or corn
Dislocation
Flatfoot
Fracture
Gout
Hallux rigidus
Hammer toe
Ingrown toenail
Köhler’s disease
Morton’s neuroma
Occlusive vascular disease
Plantar fasciitis
Plantar wart
Radiculopathy
Tabes dorsalis
Tarsal tunnel syndrome
♦ Compartment syndrome. Progressive, intense lower leg pain that increases with passive muscle stretching is a cardinal sign of this limbthreatening disorder. Restrictive dressings or traction may aggravate the pain, which typically worsens despite analgesic administration. Other findings include muscle weakness and paresthesia, but apparently normal distal circulation. With irreversible muscle ischemia, paralysis and absent pulse also occur.
♦ Fracture. Severe, acute pain accompanies swelling and ecchymosis in the affected leg. Movement produces extreme pain, and the leg may be unable to bear weight. Neurovascular status distal to the fracture may be impaired, causing paresthesia, absent pulse, mottled cyanosis, and cool skin. Deformity, muscle spasms, and bony crepitation may also occur.
♦ Infection. Local leg pain, erythema, swelling, streaking, and warmth characterize soft-tissue and bone infections. Fever and tachycardia may be present with other systemic signs.
♦ Multiple myeloma. Pain that begins in the ribs or lower back and progresses to the hips and legs may be a symptom of advanced multiple myeloma. Other signs and symptoms may include kidney problems, fatigue, and recurrent infections.
♦ Occlusive vascular disease. Continuous cramping pain in the legs and feet may worsen with walking, inducing claudication. The patient may report increased pain at night, cold feet, cold intolerance, numbness, and tingling. Examination may reveal ankle and lower leg edema, decreased or absent pulses, and increased capillary refill time. (Normal time is less than 3 seconds.)
♦ Sciatica. Pain, described as shooting, aching, or tingling that radiates down the back of the leg along the sciatic nerve. Typically, activity exacerbates the pain and rest relieves it. The patient may limp to avoid exacerbating the pain and may have difficulty moving from a sitting to a standing position.
♦ Strain or sprain. Acute strain causes sharp, transient pain and rapid swelling, followed by leg tenderness and ecchymosis. Chronic strain produces stiffness, soreness, and generalized leg tenderness several hours after the injury; active and passive motion may be painful or impossible. A sprain causes local pain, especially during joint movement; ecchymosis and, possibly, local swelling and loss of mobility develop.
♦ Thrombophlebitis. Discomfort may range from calf tenderness to severe pain accompanied by swelling, warmth, and a feeling of heaviness in the affected leg. The patient may also develop fever, chills, malaise, muscle cramps, and a positive Homans’ sign. Assessment may reveal superficial veins that are visibly engorged; palpable, hard, thready, and cordlike; and sensitive to pressure.
♦ Varicose veins. Mild to severe leg symptoms may develop, including nocturnal cramping; a feeling of heaviness; diffuse, dull aching after prolonged standing or walking; and aching during menses. Assessment may reveal palpable nodules, orthostatic edema, and stasis pigmentation of the calves and ankles.
Primary varicose veins originate in the superficial system and are more common in women.
♦ Venous stasis ulcers. Localized pain and bleeding arise from infected ulcerations on the lower extremities. Mottled, bluish pigmentation is characteristic, and local edema may occur.
SPECIAL CONSIDERATIONS
If the patient has acute leg pain, closely monitor his neurovascular status by frequently checking distal pulses and evaluating both legs for temperature, color and sensation. Also monitor his thigh and calf circumference to evaluate bleeding into tissues from a possible fracture site. Prepare him for X-rays. Use sandbags to immobilize his leg; apply ice and, if needed, skeletal traction. If a fracture isn’t suspected, prepare the patient for laboratory tests to detect an infectious agent or for venography, Doppler ultrasonography, plethysmography, or angiography to determine vascular competency. Withhold food and fluids until the need for surgery has been ruled out, and withhold analgesics until a preliminary diagnosis is made. Administer an anticoagulant and antibiotic as needed.
PEDIATRIC POINTERS
Common pediatric causes of leg pain include fracture, growing pains, osteomyelitis, and bone cancer. If parents fail to give an adequate explanation for a leg fracture, consider the possibility of child abuse.
PATIENT COUNSELING
If the patient has chronic leg pain, instruct him to take an anti-inflammatory and teach him to perform range-of-motion exercises and, if necessary, to use a cane, walker, or other assistive device. Discuss with the patient and his family any lifestyle changes that may be necessary until leg pain resolves. If physical therapy is necessary, stress the importance of establishing a daily exercise regimen. Based on the cause of the leg pain, discuss the appropriate positioning of the lower extremity to enhance blood flow and venous return.
Level of consciousness, decreased
A decrease in level of consciousness (LOC), from lethargy to stupor to coma, usually results from a neurologic disorder and may signal a life-threatening complication, such as hemorrhage, trauma, or cerebral edema. However, this sign can also result from a metabolic, GI, musculoskeletal, urologic, or cardiopulmonary disorder; severe nutritional deficiency; the effects of toxins; or drug use. LOC can deteriorate suddenly or gradually and can remain altered temporarily or permanently.
Consciousness is affected by the reticular activating system (RAS), an intricate network of neurons with axons extending from the brain stem, thalamus, and hypothalamus to the cerebral cortex. A disturbance in any part of this integrated system prevents the intercom-munication that makes consciousness possible. Loss of consciousness can result from a bilateral cerebral disturbance, an RAS disturbance, or both. Cerebral dysfunction characteristically produces the least dramatic decrease in a patient’s LOC. In contrast, dysfunction of the RAS produces the most dramatic decrease in LOC—coma.
The most sensitive indicator of decreased LOC is a change in the patient’s mental status. The Glasgow Coma Scale, which measures a patient’s ability to respond to verbal, sensory, and motor stimulation, can be used to quickly evaluate a patient’s LOC.
After evaluating the patient’s airway, breathing, and circulation, use the Glasgow Coma Scale to quickly determine his LOC and to obtain baseline data. (See Using the Glasgow Coma Scale, page 422.) If the patient’s score is 13 or less, emergency surgery may be necessary. Insert an artificial airway, elevate the head of the bed 30 degrees and, if spinal cord injury has been ruled out, turn the patient’s head to the side. Prepare to suction the patient if necessary. You may need to hyperventilate him to reduce carbon dioxide levels and decrease intracranial pressure (ICP). Then determine the rate, rhythm, and depth of spontaneous respirations. Support his breathing with a handheld resuscitation bag, if necessary. If the patient’s Glasgow Coma Scale score is 7 or less, intubation and resuscitation may be necessary.
Continue to monitor the patient’s vital signs, being alert for signs of increasing ICP, such as bradycardia and widening pulse pressure. When his airway, breathing, and circulation are stabilized, perform a neurologic examination.
HISTORY AND PHYSICAL EXAMINATION
Try to obtain history information from the patient, if he’s lucid, and from his family. Did the patient complain of headache, dizziness, nausea, visual or hearing disturbances, weakness, fatigue, or any other problems before his LOC decreased? Has his family noticed any changes in the patient’s behavior, personality, memory, or temperament? Also ask about a history of neurologic disease, cancer, or recent trauma or infections; drug and alcohol use; and the development of other signs and symptoms.
Because decreased LOC can result from a disorder affecting virtually any body system, tailor the remainder of your evaluation according to the patient’s associated symptoms.
MEDICAL CAUSES
♦ Adrenal crisis. Decreased LOC, ranging from lethargy to coma, may develop within 8 to 12 hours of onset. Early associated findings include progressive weakness, irritability, anorexia, headache, nausea and vomiting, diarrhea, abdominal pain, and fever. Later signs and symptoms include hypotension; rapid, thready pulse; oliguria; cool, clammy skin; and flaccid extremities. The patient with chronic adrenocortical hypofunction may have hyperpigmented skin and mucous membranes.
♦ Brain abscess. Decreased LOC varies from drowsiness to deep stupor, depending on abscess size and site. Early signs and symptoms— constant intractable headache, nausea, vomiting, and seizures—reflect increasing ICP. Typical later features include ocular disturbances (nystagmus, vision loss, and pupillary inequality) and signs of infection such as fever. Other findings may include personality changes, confusion, abnormal behavior, dizziness, facial weakness, aphasia, ataxia, tremor, and hemiparesis.
♦ Brain tumor. LOC decreases slowly, from lethargy to coma. The patient may also experience apathy, behavior changes, memory loss, decreased attention span, morning headache, dizziness, vision loss, ataxia, and sensorimotor disturbances. Aphasia and seizures are possible, along with signs of hormonal imbalance, such as fluid retention or amenorrhea. Signs and symptoms vary according to the location and size of the tumor. In later stages, papilledema, vomiting, bradycardia, and widening pulse pressure also appear. In the final stages, the patient may exhibit decorticate or decerebrate posture.
♦ Cerebral aneurysm (ruptured). Somnolence, confusion and, at times, stupor characterize a moderate bleed; deep coma occurs with severe bleeding, which can be fatal. Onset is usually abrupt, with sudden, severe headache, nausea, and vomiting. Nuchal rigidity, back and leg pain, fever, restlessness, irritability, occasional seizures, and blurred vision point to meningeal irritation. The type and severity of other findings vary with the site and severity of the hemorrhage and may include hemiparesis, hemisensory defects, dysphagia, and visual defects.
♦ Cerebral contusion. Usually unconscious for a prolonged period, the patient may develop dilated, nonreactive pupils and decorticate or decerebrate posture. If he’s conscious or recovers consciousness, he may be drowsy, confused, disoriented, agitated, or even violent. Associated findings include blurred or double vision, fever, headache, pallor, diaphoresis, tachycardia, altered respirations, aphasia, and hemiparesis. Residual effects include seizures, impaired mental status, slight hemiparesis, and vertigo.
Using the Glasgow Coma Scale
The Glasgow Coma Scale describes a patient’s baseline mental status and helps to detect and interpret changes from baseline findings. When using the Glasgow Coma Scale, test the patient’s ability to respond to verbal, motor, and sensory stimulation, and grade your findings according to the scale. A score of 15 indicates that the patient is alert, can follow simple commands, and is oriented to time, place, and person. A decreased score in one or more categories may signal an impending neurologic crisis. A score of 7 or less indicates severe neurologic damage.
Test
Score
Response
Eye-opening response
Spontaneously
4
Opens eyes spontaneously
To speech
3
Opens eyes when told to
To pain
2
Opens eyes only to painful stimulus
None
1
Doesn’t open eyes in response to stimuli
Motor response
Obeys
6
Shows two fingers when asked
Localizes
5
Reaches toward painful stimulus and tries to remove it
Withdraws
4
Moves away from painful stimulus
Abnormal flexion
3
Assumes a decorticate posture (shown below)
Abnormal extension
2
Assumes a decerebrate posture (shown below)
None
1
No response; just lies flaccid (an ominous sign)
Verbal response (to question, “What year is this?”)
Oriented
5
Tells correct year
Confused
4
Tells incorrect year
Inappropriate words
3
Replies randomly with incorrect words
Incomprehensible
2
Moans or screams
No response
1
No response
Total score
(3 to 15)
♦ Diabetic ketoacidosis. This disorder produces a rapid decrease in LOC, ranging from lethargy to coma, commonly preceded by polydipsia, polyphagia, and polyuria. The patient may complain of weakness, anorexia, abdominal pain, nausea, and vomiting. He may also exhibit orthostatic hypotension; fruity breath odor; Kussmaul’s respirations; warm, dry skin; and a rapid, thready pulse. Untreated, this condition invariably leads to coma and death. ♦ Encephalitis. Within 24 to 48 hours after onset, the patient may develop LOC changes ranging from lethargy to coma. Other possible findings include abrupt onset of fever, headache, nuchal rigidity, nausea, vomiting, irritability, personality changes, seizures, aphasia, ataxia, hemiparesis, nystagmus, photophobia, myoclonus, and cranial nerve palsies.
♦ Encephalomyelitis (postvaccinal). This life-threatening disorder produces rapid LOC deterioration from drowsiness to coma. The patient also experiences rapid onset of fever, headache, nuchal rigidity, back pain, vomiting, and seizures.
♦ Encephalopathy. With hepatic encephalopathy, signs and symptoms develop in four stages: in the prodromal stage, slight personality changes (disorientation, forgetfulness, slurred speech) and slight tremor; in the impending stage, tremor progressing to asterixis (the hallmark of hepatic encephalopathy), lethargy, aberrant behavior, and apraxia; in the stuporous stage, stupor and hyperventilation, with the patient noisy and abusive when aroused; in the comatose stage, coma with decerebrate posture, hyperactive reflexes, positive Babinski’s reflex, and fetor hepaticus.
With life-threatening hypertensive encephalopathy, LOC progressively decreases from lethargy to stupor to coma. Besides markedly elevated blood pressure, the patient may experience severe headache, vomiting, seizures, visual disturbances, transient paralysis, and eventually Cheyne-Stokes respirations.
With hypoglycemic encephalopathy, LOC rapidly deteriorates from lethargy to coma. Early signs and symptoms include nervousness, restlessness, agitation, and confusion; hunger; alternate flushing and cold sweats; and headache, trembling, and palpitations. Blurred vision progresses to motor weakness, hemiplegia, dilated pupils, pallor, decreased pulse rate, shallow respirations, and seizures. Flaccidity and decerebrate posture appear late.
Depending on its severity, hypoxic encephalopathy produces a sudden or gradual decrease in LOC, leading to coma and brain death. Early on, the patient appears confused and restless, with cyanosis and increased heart and respiratory rates and blood pressure. Later, his respiratory pattern becomes abnormal, and assessment reveals decreased pulse, blood pressure, and deep tendon reflexes (DTRs); Babinski’s reflex; absent doll’s eye sign; and fixed pupils.
With uremic encephalopathy, LOC decreases gradually from lethargy to coma. Early on, the patient may appear apathetic, inattentive, confused, and irritable and may complain of headache, nausea, fatigue, and anorexia. Other findings include vomiting, tremors, edema, papilledema, hypertension, cardiac arrhythmias, dyspnea, crackles, oliguria, and Kussmaul’s and Cheyne-Stokes respirations.
♦ Epidural hemorrhage (acute). This life-threatening posttraumatic disorder produces momentary loss of consciousness, sometimes followed by a lucid interval. While lucid, the patient has a severe headache, nausea, vomiting, and bladder distention. Rapid deterioration in consciousness follows, possibly leading to coma. Other findings include irregular respirations, seizures, decreased and bounding pulse, increased pulse pressure, hypertension, unilateral or bilateral fixed and dilated pupils, unilateral hemiparesis or hemiplegia, decerebrate posture, and Babinski’s reflex.
♦ Heatstroke. As body temperature increases, LOC gradually decreases from lethargy to coma. Early signs and symptoms include malaise, tachycardia, tachypnea, orthostatic hypotension, muscle cramps, rigidity, and syncope. The patient may be irritable, anxious, and dizzy and may report a severe headache. At the onset of heatstroke, the patient’s skin is hot, flushed, and diaphoretic with blotchy cyanosis; later, when his fever exceeds 105° F (40.5° C), his skin becomes hot, flushed, and anhidrotic. Pulse and respiratory rate increase markedly, and blood pressure drops precipitously. Other findings include vomiting, diarrhea, dilated pupils, and Cheyne-Stokes respirations.
Only gold members can continue reading. Log In or Register to continue
 If the patient has acute leg pain and a history of trauma, quickly take his vital signs and determine the leg’s neurovascular status. Observe the patient’s leg position and check for swelling, gross deformities, or abnormal rotation. Also, be sure to check distal pulses and note skin color and temperature. A pale, cool, and pulseless leg may indicate impaired circulation, which may require emergency surgery.
If the patient has acute leg pain and a history of trauma, quickly take his vital signs and determine the leg’s neurovascular status. Observe the patient’s leg position and check for swelling, gross deformities, or abnormal rotation. Also, be sure to check distal pulses and note skin color and temperature. A pale, cool, and pulseless leg may indicate impaired circulation, which may require emergency surgery.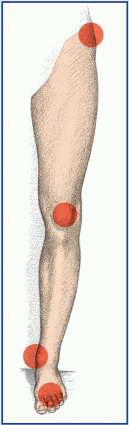
 Primary varicose veins originate in the superficial system and are more common in women.
Primary varicose veins originate in the superficial system and are more common in women. After evaluating the patient’s airway, breathing, and circulation, use the Glasgow Coma Scale to quickly determine his LOC and to obtain baseline data. (See Using the Glasgow Coma Scale, page 422.) If the patient’s score is 13 or less, emergency surgery may be necessary. Insert an artificial airway, elevate the head of the bed 30 degrees and, if spinal cord injury has been ruled out, turn the patient’s head to the side. Prepare to suction the patient if necessary. You may need to hyperventilate him to reduce carbon dioxide levels and decrease intracranial pressure (ICP). Then determine the rate, rhythm, and depth of spontaneous respirations. Support his breathing with a handheld resuscitation bag, if necessary. If the patient’s Glasgow Coma Scale score is 7 or less, intubation and resuscitation may be necessary.
After evaluating the patient’s airway, breathing, and circulation, use the Glasgow Coma Scale to quickly determine his LOC and to obtain baseline data. (See Using the Glasgow Coma Scale, page 422.) If the patient’s score is 13 or less, emergency surgery may be necessary. Insert an artificial airway, elevate the head of the bed 30 degrees and, if spinal cord injury has been ruled out, turn the patient’s head to the side. Prepare to suction the patient if necessary. You may need to hyperventilate him to reduce carbon dioxide levels and decrease intracranial pressure (ICP). Then determine the rate, rhythm, and depth of spontaneous respirations. Support his breathing with a handheld resuscitation bag, if necessary. If the patient’s Glasgow Coma Scale score is 7 or less, intubation and resuscitation may be necessary.