Juvenile Xanthogranuloma
Key Facts
Terminology
Abbreviation:
Pulmonary juvenile xanthogranuloma (JXG)
Definition
Non-Langerhans histiocytic lesion
Etiology/Pathogenesis
Contrary to other histiocytic lesions, cell of origin for JXG is unknown
Plasmacytoid monocyte has been speculated as possible origin for JXG
Clinical Issues
Presentation
Bilateral or unilateral involvement of lung parenchyma
Multiple pulmonary lesions
Rarely, lesion will be single
Dermal involvement is common
Involvement of other organ systems may occur
Microscopic Pathology
Cellular proliferation destroying lung parenchyma
Histocytes admixed with inflammatory infiltrate composed of lymphocytes and plasma cells
Multinucleated giant cells may be present but scattered
Absence of nuclear atypia or mitotic activity
Top Differential Diagnoses
Langerhans cell histiocytosis (LCH)
Rosai-Dorfman disease of lung
Erdheim-Chester disease
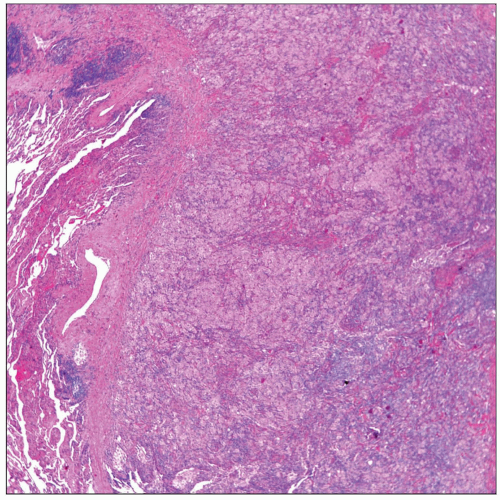 Low-power view of a JXG shows replacement of the lung parenchyma by a histiocytic proliferation admixed with inflammatory infiltrate. |
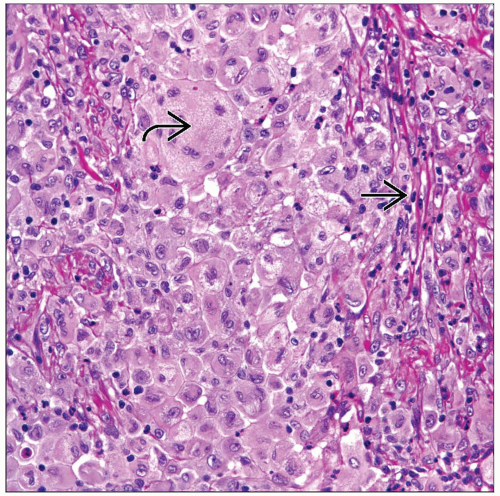 High-power view of the histiocytic proliferation shows large histiocytes  with round nuclei and prominent nucleoli. A subtle inflammatory infiltrate is also present with round nuclei and prominent nucleoli. A subtle inflammatory infiltrate is also present  . . |
TERMINOLOGY
Abbreviations
Pulmonary juvenile xanthogranuloma (JXG)
Definitions
Non-Langerhans histiocytic lesion
ETIOLOGY/PATHOGENESIS
Etiology
Contrary to other histiocytic lesions, cell of origin for JXG is unknown
Plasmacytoid monocyte has been speculated as possible origin for JXG
CLINICAL ISSUES
Presentation
Bilateral or unilateral involvement of lung parenchyma
Multiple pulmonary lesions
Rarely, lesion will be single
Dermal involvement is common
Involvement of other organ systems may occur
Treatment
Surgical approaches
Complete surgical resection, if that can be accomplished
Prognosis
Due to rarity of this lesion in lung, it is difficult to unequivocally determine prognosis
May be determined by extent of the process
MACROSCOPIC FEATURES
General Features
Tumor mass can range in size from 1-3 cm
Well circumscribed but not encapsulated
Soft and tan or yellowish in color
MICROSCOPIC PATHOLOGY
Histologic Features
Cellular proliferation destroying lung parenchyma
Histiocytic proliferation composed of small to medium-sized histiocytes
Histocytes admixed with inflammatory infiltrate composed of lymphocytes and plasma cells
Multinucleated giant cells may be present but scattered
Absence of nuclear atypia or mitotic activity
DIFFERENTIAL DIAGNOSIS
Langerhans Cell Histiocytosis (LCH)
Lesions in LCH may vary from cellular to fibrotic
Presence of large number of eosinophils is more common in LCH
Histiocytes have characteristic “grooving” of nucleus
LCH lesions have characteristic “Medusa’s head,” which is not present in JXG
Usually associated with diffuse interstitial pneumonia-like reaction in adjacent lung parenchyma
Positive for CD1a and S100
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


