Joint replacement surgery represents one of the most successful medical advances of the 20th century and has shown a logarithmic growth in use as the U.S. population ages. The Swedish Hip Registry has documented the diagnosis at the time of primary joint replacements in Sweden at different age groups (1) (Table 17.1). Although 25-year rates of survivorship for hip replacement free of reoperation have been estimated as high as 77 percent (2), joint replacements are not expected to last forever, and the reasons for revisions have been increasingly documented (Table 17.2).
With the advent of orthopaedic implants in treating a wide variety of joint diseases, complications have been increasingly studied and carefully documented (Table 17.3). Nonspecific problems related to this level of surgery range from deep vein thrombosis and pulmonary embolism (2,3) to other commonly described complications, such as postoperative infections, nerve palsies, and even death (4). Mortality rates after total hip replacement within 30 to 90 days after surgery have been reported at 0.45 percent. The more specific effects of implants on native tissue are of special concern, and a range of problems have been documented including anatomical, mechanical, and biologic complications (5,6) (Table 17.3). These include, most significantly, loosening of the prosthesis.
Under certain circumstances, significant osteolysis (7), bone-resorbing fibrous pseudoarthrotic membranes (8), and granulomatous reactions may occur (9). Localized and disseminated granulomatous reactions to implant materials in regional and distant lymph nodes are now well described (10), with the shortest interval between joint implantation and dissemination of metal to a lymph node chain estimated at 6 months (11). Effects on other tissues, including the liver and spleen, have also been documented.
Autopsy reports have established that wear particles travel to the liver and spleen and may do so by hematogenous spread (12,13). Although the pathologic consequences, if any, are hard to assess, the presence of granulomatous reactions to wear particles in the liver suggests that possibility.
Foreign body reactions may or may not be granulomatous and have been described to mimic sarcoidosis and even sarcomas. Indeed, carcinomas, sarcomas, and even lymphomas of bone have been reported in association with implants (14). To date, however, the incidence is rare and a direct etiologic link doubtful. The creation of registries to report such associations has been urged (vide infra “implant sarcomas”).
Self-reporting registries by surgeons of their complications and outcomes have been found to play an important role in the early identification of problems. International joint registries initially focused on arthroplasty revision rates, but have broadened their focus to include perioperative complications and patient-reported outcomes (14). The recent recall of metal-on-metal implants has emphasized the importance of registries as countries with registries recognized the associated adverse local tissue reactions earlier than those countries without such reporting. The United States, late to the development of a registry, has begun pilot programs that will hopefully function as useful surveillance tools to assess both postoperative events and patient pain relief, function, and revision rates.
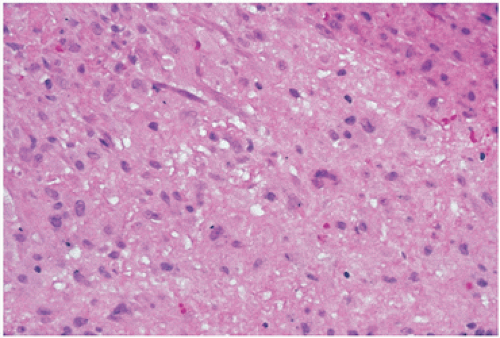
Registries in Sweden have allowed Sweden to have a rate of revision hip replacement surgery to be 8 percent compared with 18 percent in the United States (15). In addition, approximately 50 percent of devices approved for introduction to the orthopaedic marketplace are no longer available 10 years later (16). Although one can suspect under documentation of complications as a factor, the competitive marketplace plays a role, with issues such as company takeovers and slow sales being factors. Recalls are also a factor, with one highly celebrated recall leading to the financial collapse of a major company. In the celebrated Sulzer Inter-Op failure, a previously successful hip socket implant was found to cause persistent pain. The problem was eventually traced to a processing step that had been eliminated when a transfer of the production of the implant was made to another factory from an outside contractor. An acid bath step in the processing had been eliminated, resulting in loss of a protective effect on removing mineral oil residue. The resultant reoperations for lack of fixation were attributed to residual mineral oil (Fig. 17.1). Such catastrophic failures have led to guidelines outlining the responsibilities of surgeons (and pathologists) when confronting a defective surgical implant (17). These include notification of the hospital, the Food and Drug Administration, the manufacturer, and, most importantly, the patient.
TABLE 17.1 Diagnosis at the Time of the Initial Operation (1992 to 2003)
Patients Younger than 50 y
Patients 50-59 y
Patients 60-75 y
Patients Older than 75 y
Total
Diagnoses
Number
Percent
Number
Percent
Number
Percent
Number
Percent
Number
Percent
Primary osteoarthritis
3,129
52.0
13,067
78.2
51,775
80.5
27,584
66.9
95,555
74.5
Fracture
207
3.4
686
4.1
5,106
7.9
8,658
21.0
14,657
11.4
Inflammatory disease
1,058
17.6
1,140
6.8
2,770
4.3
927
2.2
5,895
4.6
Avascular necrosis
374
6.2
456
2.7
1,298
2.0
1569
3.8
3,697
2.9
Childhood disease
762
12.7
636
3.8
489
0.8
116
0.3
2,003
1.6
Secondary osteoarthritis
95
1.6
110
0.7
469
0.7
619
1.5
1,293
1.0
Tumor
71
1.2
127
0.8
234
0.4
125
0.3
557
0.4
Traumatic osteoarthritis
51
0.8
48
0.3
121
0.2
115
0.3
335
0.3
Missing diagnoses
274
1.6
437
2.6
2,094
3.3
1,542
3.7
4,347
3.4
Total
6,021
100
16,707
100
64,356
100
41,255
100
128,339
100
Reprinted with permission from Malchau H, Garellick G, Eisler T, et al. The Swedish hip registry. Clin Orthop. 2005;441:19-29.
Of all the complications observed, orthopaedic research and clinical attention has focused on the pain and/or loosening of the prosthesis due to osteolysis associated with wear debris and periprosthetic joint infection. Immunologic reactions and carcinogenesis remain of interest and of theoretical concern, but to date have not been either well documented or substantially linked to significant clinical pathology.
In general, revision failure rates are higher (18) and occur sooner than primary joint replacement procedures, and are more commonly associated with diagnoses of rheumatoid arthritis, diabetes mellitus, obesity, and the use of glucocorticoids (19).
Loosening
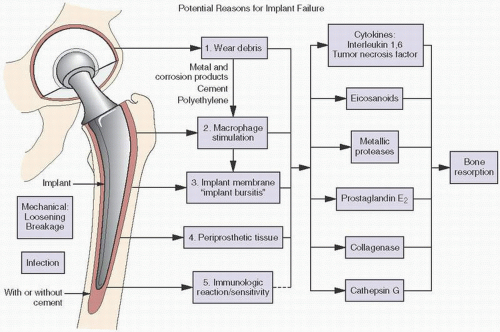
A significant complication of implantation is micromotion and subsequent loosening of the prosthesis, which may be caused by both biologic and mechanical factors (Table 17.4, Fig. 17.2). Loosening has been estimated to occur in as many as 50 percent of cemented total hip replacements followed for more than 10 years, but can be a sequela of uncemented procedures as well. Mechanical instability may result from excessive activity by the patient or material failures. Biologic causes of loosening include infection and inflammation, the latter usually macrophage-mediated, reactions to debrided particulate matter from joint components. Osteolysis, which may follow all the previously mentioned factors, is another significant cause in that it perpetuates the cycle of loosening (Fig. 17.3).
There also is evidence that intracapsular pressure raised by the surgical procedure itself induces osteolysis (20). For example, the elevated intracapsular pressure that can accompany a hip with loose components may, by pressure, pump debris along interfaces and in and of itself cause osteolysis and loosening (21).
Bacterial endotoxins have also been proposed as a mechanism promoting loosening by modulating the biologic response to wear particles. Substances such as lipopolysaccharide from gram-negative organisms or lipoteichoic acid, and peptidoglycan from gram-positive organisms may originate from otherwise harmless and subclinical intestinal flora, minor infections, and dental procedures, and attach to wear particles acting synergistically to promote osteolysis (22).
Immunologically, metallic ions can serve as haptens and may elicit an adaptive immune response (23). Commonly used alloy metals, for example, nickel, cobalt, chromium, and, rarely, others such as titanium have been implicated as relevant allergens.
Patch-test sensitivity to metals in the normal population is estimated at 10 percent, with nickel, a common component of inexpensive jewelry, far more “allergic” than cobalt or chromium. In functioning implants, it has been assessed as high as 25 percent, and in a loosened implant, >60 percent. Extreme reactivity to metal, however, is unusual and estimated at approximately 1 percent of the population. Chronically loose implants with their associated metallic debris may sensitize persons who were previously without sensitivity. However, significant immunologic reactions, including dermatitis and eczema, have not been widely reported.
TABLE 17.2 Reason for Revision (1979 to 2003) in Sweden
0 Revisions
1 Revision
2 Revisions
More than 2 Revisions
Total
Reason for Revision
Number
Percent
Number
Percent
Number
Percent
Number
Percent
Number
Percent
Aseptic loosening
13,581
76.0
1,829
64.4
319
61.3
59
46.8
15,788
73.9
Infection
1,292
7.2
316
11.1
64
12.3
26
20.6
1,698
7.9
Dislocation
1,176
6.6
325
11.4
69
13.3
27
21.4
1,597
7.5
Periprosthetic fracture
996
5.4
221
7.8
38
7.3
2
1.6
1,227
5.7
Technical reason
447
2.5
71
2.5
17
3.3
2
1.6
537
2.5
Implant fracture
276
1.5
45
1.6
7
1.3
3
2.4
331
1.5
Miscellaneous
86
0.5
24
0.8
5
1.0
6
4.8
121
0.6
Pain only
57
0.3
9
0.3
1
0.2
1
0.8
68
0.3
Total
17,881
100
2,840
100
520
100
126
100
21,367
100
Reprinted with permission from Malchau H, Garellick G, Eisler T, et al. The Swedish hip registry. Clin Orthop. 2005;441:19-29.
It would nonetheless appear prudent to advise a patient who has a known dermal allergy to jewelry that such a reaction can attenuate the normal life span of the joint replacement.
Clinical criteria for “loosening” vary, and although many criteria have been postulated, there is still no general consensus on what constitutes clinically significant loosening.
Factors that may contribute to failure or loosening include wear fatigue of the materials used, debonding between tissue or implant interface planes (which further creates an environment for corrosion), and fatigue damage and wear secondary to radiation techniques used to sterilize implants. Both adhesive forces that literally pull wear particles from surfaces, and abrasive actions that occur between soft and hard elements of the implant may be further contributory factors (24).
In hips, osteolysis-associated loosening usually appears about 4 years after surgery. Sixty percent of lesions progress, with progression occurring slowly at about 0.89 mm/year.
Osteolysis
Activation of macrophages by wear debris initiated by subclinically evident micromotion (25) is considered the leading cause of osteolysis (Fig. 17.4). However, wear debris may also be the result of many fundamental mechanisms of wear (26).
In order to bring clarity to the plethora of terms used to describe wear, McKellop et al. have proposed four categories of wear:
Wear “Modes” refer to the in vivo conditions under which the wear occurred;
Wear “Mechanisms” refer to fundamental wear processes (adhesion, abrasion, fatigue, and tribochemical reactions):
Wear “Damage” refers to the resultant changes in the morphology and/or composition of the surfaces; and
Wear “Features” refer to the specific wear phenomena that are described in terms of the relevant modes, mechanisms, and damage.
In addition, the term corrosion refers to electrochemical processes that can remove or add material and thus also generate damage. Corrosion can act alone or may interact with mechanical wear (26).
As defined by Bauer and Schils (27), adhesive wear results from transient bonding between the articulating surface under load, which may extract particles from the weaker surface. Abrasive wear occurs when surfaces of different hardness create a scratching effect. Fatigue wear occurs when accumulated stresses on the surface of an implant exceed intrinsic fatigue strength. Modes of wear include that between two surfaces or between two surfaces with an interposed third party particle such as bone, cement, metal, or polyethylene (PE).
TABLE 17.3 Pathology Associated with Joint Implants
a The three most common reasons for revision of a total hip replacement.
Corrosion products can be generated from metal ions released from an implant surface, especially in metal-on-metal implants. Wear damage may be grossly visible as scratching, burnishing, delamination, and/or pitting (Fig. 17.5).
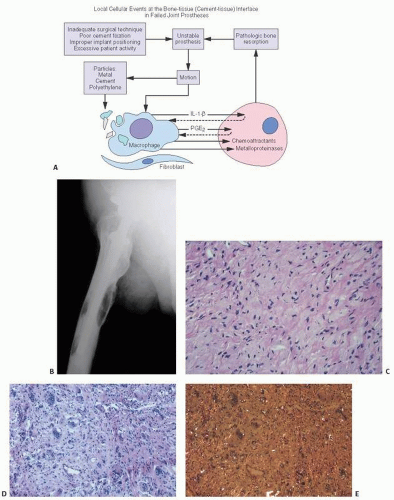
FIGURE 17.1. Failed prosthesis due to manufacturing procedural change: tissue showed vacuolar oily spaces consistent with remnants of contaminant oil-based residue not removed when a processing step was mistakenly deleted in the manufacturer’s protocol (hematoxylin and eosin).
TABLE 17.4 Major Causes of Loosening of Joint Implants
1.
Mechanical factors
Material failure
Patient activity: mechanical loosening
Implant size or fit (e.g., small femoral head)
2.
Osteolysis
3.
Infection
4.
Inflammatory reactions to prosthetic wear debris
Polyethylene
Polymethylmethacrylate cement
Metal
Silicone
Important characteristics of wear include wear rates roughly estimated at 0.14 mm/year for cobalt-chromium and 0.10 mm/year for PE. Wear rates above 0.2 mm/year may be a critical level above which patients are at risk for wear-related complications. Most wear debris is <1 µm in size, often below the detectable limit on transmission light microscopy, with the mean size of a PE particle 0.5 µm. Thus, there are certainly more wear particles than apparent to the routine diagnostic pathologist. Particulate size dictates the pathologic reaction (28). Particles <7 µm are phagocytosable by mononuclear macrophages, larger ones by foreign body giant cells, and those much larger (mean, 67 µm) encapsulated by fibrosis (26). Bioreactivity of particulate debris is also related to composition and concentration. Because it has been estimated that billions of particles are produced during the life of an implant, the sheer scope of possible particle-induced pathology is substantial.
Macrophages engulf particulate wear debris (PE more than metal or cement) from prosthetic materials and release. Proinflammatory factors include:
In addition, the NOD-like receptor protein, NALP3, located in macrophages initiates cleavage of pro-IL1 β into its secreted form, triggering an inflammatory cascade (31). The specific nature of the macrophage response depends on many parameters including the composition, size, shape, volume, and surface area of the particulate debris.
These can mediate the differentiation of osteoclast precursor cells and activate mature osteoclasts. The complicated role played by substances such as IL-6 and interferon-α is underscored by some studies that demonstrate wear debris inhibition of the antiosteoclastogenic signaling of these molecules (32). Recent investigations have focused on the role of blockading the osteoclast activation path by interfering with RANKL (the receptor activator of NF-κB) (33).
RANKL is expressed on the cell surfaces of osteoblasts and bone marrow stromal cells, and it can stimulate the differentiation of osteoclast progenitor cells to form mature osteoclasts. This signaling is mediated through a receptor/activator termed RANK, which is located on the cell membrane of osteoclast precursors and mature osteoclasts (34).
FIGURE 17.2. Factors leading to loosening of an implant.
A third molecule, osteoprotegerin, which negatively regulates this process by inhibiting RANK’s capacity to activate RANKL, may reflect a protective effect against osteolysis if shown to be elevated in serum (35).
Wear debris particles may be opsonized by host proteins and substances such as albumin, collagen, and fibronectin. Antibodies may introduce alterations in surface charges or composition, which affect local cellular activity (25). The additional role of bacterial products, such as endotoxin, remains unclear.
Wear debris may also activate osteoblasts, lymphocytes, synoviocytes, and fibroblasts with resultant proinflammatory cytokine activation and activation of metalloproteinases, stromelysin, and collagenase, a virtual alphabet soup of tissue resorptive substances (36). The levels of cathepsins in interface tissue have been measured at higher than that in rheumatoid synovium (37).
There are few, if any, laboratory markers that can indicate or correlate with the osteolysis around implants or the associated increased bone remodeling. Despite the fact that some studies have attempted to correlate loosening with increases in circulating cytokines (such as IL-1 or IL-6) (30,38) or in bone remodeling serum markers such as cross-linked N-terminal telopeptide (NTX) and procollagen I C-terminal extension peptide (PICP), the current diagnosis of aseptic loosening remains clinical and radiologic (39,40).
In summary, osteolysis can be seen as the end result of a number of mechanisms, including:
Wear debris-induced macrophage stimulation
Elevated intra-articular pressure
Micromotion
Possibly hypersensitivity
Whatever the cause of osteolysis, it may be first evidenced by pain or the appearance of radiolucent lines, zones, or regions between the implant or implantable material and the host bone (Fig. 17.6).
Implant-associated Membranes
In the ideal situation, the introduction of an implant and the subsequent reaming of the bone for implant placement would lead to healing, not unlike that seen in normal fracture healing. The implant would stimulate the differentiation of osteoblasts in adjacent tissue, with eventual osseous anchorage. In actual practice, however, micromotion may lead to fibrosis rather than bone, the final result being the formation of a fibrous or, in some instances, synovial and bursa-like membrane, similar to that seen in pseudoarthroses (Fig. 17.7).
Clinically and roentgenographically, this fibrous membrane may appear as a loose prosthesis with a radiolucent line at the implant-bone interface (Fig. 17.6). However, radiolucency does not necessarily mean clinical loosening. In general, it seems difficult to establish a clear correlation between radiographic and clinical loosening. Indeed, radiolucent zones between implants and host tissue may be either physiologic or pathologic (41).
The accuracy of comparing different imaging modalities in the detection of osteolysis has been studied extensively. In a cadaveric model, the sensitivity for detecting lesions was 51.7 percent for computed tomography and 95.4 percent for magnetic resonance imaging (MRI) (42).
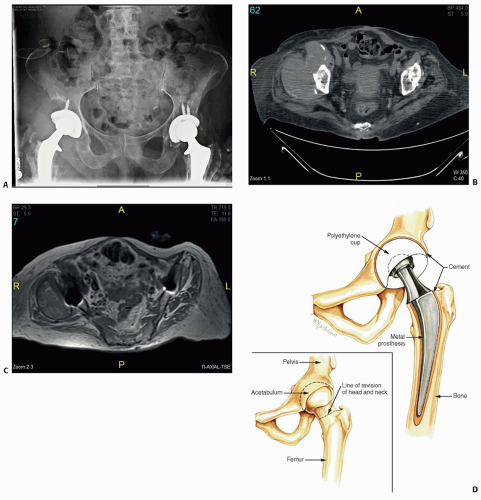
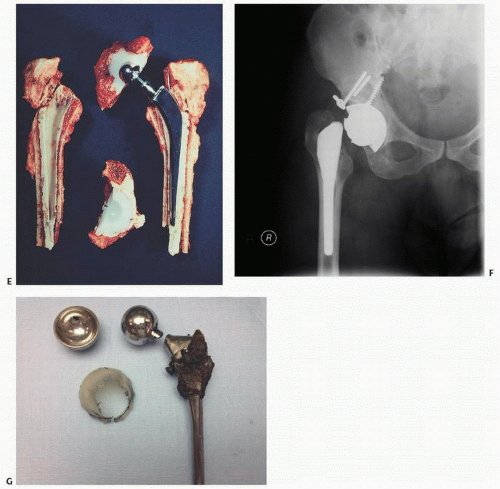
FIGURE 17.3. (A) Roentgenograph showing loosened hip implant with significant bone loss (osteolysis). Grossly, the hardware components that may individually or collectively lead to tissue pathology are the metal prosthesis itself, the polyethylene (plastic) component, or the fixation cement (polymethylmethacrylate), if used. (B) Axial CT image showing large soft tissue mass around the right acetabulum. (C) Axial MRI with a large mass demonstrating a low T1 signal. (D) Artist rendering of one type of arthroplasty before and after surgery. (Continued)
When a roentgenographic radiolucency is suspected, the histologic correlation is usually that of a fibrous membrane. In a small percentage of cases, radiolucent lines have as a histologic correlation not fibrous membranes but endosteal resorption of cortical bone (43,44).
In some hip-retrieval studies, the dominant correlation of radiolucencies on the acetabular side has been fibrosis and fibrous membranes. However, in the femoral stem, endosteal bone remodeling predominates, suggesting different mechanisms at work at different anatomical sites (44).
FIGURE 17.3. (Continued) (E) Components of an arthroplasty implant removed at revision surgery. (F) Radiograph of periprosthetic fracture. (G) Removed components of a periprosthetic fracture.
Fornasier et al. (45) evaluated the bone-cement interface in successful asymptomatic total hip replacements retrieved at autopsy, and reviewed the previous understanding of the stages of development of this interface. An initial stage of postoperative tissue necrosis and damage induced by the operative procedure was followed by a second stage in which a fibroblastic ingrowth led to remodeling, repair, and replacement of the former necrotic bone. A final stage, occurring several years after implantation, led to the production of a membrane consisting of acellular, noninflammatory fibroblastic tissue. Where it was present, foreign body reactions to cement particles were thought to decrease with time. The authors concluded that the cellular constituents of the membrane include histiocytes apparently reactive to particulate PE debris, a reaction that increases with time but progresses at different rates in different patients at different sites. The histiocytic response to particulate matter may lead to healthy bone remodeling and osteoclast activation as well as macrophage handling and transportation of particulate matter away from the bone surface. This fibrous membrane, a cellular engine, may occur in both asymptomatic and symptomatic cemented arthroplasties, and both symptomatic and asymptomatic joints. Debated points included the role of micromotion in contributing to the development of the fibrous membrane and the well-known association in some patients of a marked osteolysis, aggressive granulomatous lesions, significant bone lysis, and granulomatous pseudotumors, which clearly represent an aberrant and exaggerated histiocytic and giant cell reaction to an otherwise possibly harmless reactive process (46,47,48,49). In conclusion, wear debris contributes to a cycle characterized by both histiocytic and macrophage activation and fibrous membrane proliferation.
FIGURE 17.4. Response of macrophage to particulate debris and motion, with release of bone-resorbing tissue factors and eventual osteolysis (A). Roentgenograph of implant-associated osteolysis of the femur (B). Microscopically, there may be cellular reactions composed of mononuclear histiocytes (C) and/or foreign body giant cells [light microscopy in (D), polarized light microscopy in (E)]. Usually, in reactions of this magnitude, particulate debris is evident.
FIGURE 17.5. Polyethylene implant with abrasive defects in its surface.
In one experimental model, cobalt debris was found to be toxic to fibroblasts, but particulate titanium, chromium, and titanium-aluminum alloy actually stimulated fibroblast proliferation (50). The resultant fibrous membrane was postulated to be deleterious, by acting as a conduit for transporting metallic debris and, in turn, stimulating further fibroblast- and macrophage-generated osteolysis, and thus loosening.
In a recent histopathologic study of late aseptic loosening of cemented total hip prostheses, Williams and McQueen (51) described in detail the microanatomy of implant fibrous membranes. Clinically and roentgenographically, the hip prosthesis interfaced with a densely fibrous membrane comprising three zones. The region adjacent to the cement consisted of a pseudosynovial lining, and the area immediately adjacent to that was filled with methyl methacrylate pearls, round-to-oval shaped bodies. A layer of foamy histiocytes was also noted, which ultrastructurally revealed cytoplasm filled with cellular debris and numerous lipid vacuoles. Neuronal bodies were also present, indicating that the histiocytes were phagocytosing cellular debris. In contrast, the histiocytes not in the middle layer were filled with abundant endoplasmic reticulin and protein vacuoles, these latter cells showing dense plaques and contractile filaments similar to those of myofibroblasts, suggesting that the membrane was a metaplastic response stimulated by particulate debris and motion around the loosened prosthesis. The authors concluded that late aseptic loosening is caused by fragmentation of the methyl methacrylate mantle grossly and microscopically. Methyl methacrylate particles then stimulate histiocytes adjacent to them to produce and release lytic enzymes, which in turn cause resorption of adjacent bone (51).
It is now well established that stromal cells including fibrous tissue and other inflammatory cells at the radiolucent zone may be associated with the production of potent osteolytic factors (52,53). Osteolytic factors that have been studied include IL-1α/β and TNFα, IL-6, macrophage-colony stimulating factor (M-CSF), and PGE2. In addition, fibroblasts in periprosthetic membrane tissue are capable of inducing the differentiation of normal human peripheral blood monocytes to mature osteoclasts by a mechanism that involves both RANKL and TNFα (54,55).
Macrophages may also induce bone loss directly by the release of oxide radicals and hydrogen peroxide. Clearly, giant cells and macrophages in other inflammatory conditions, such as rheumatoid arthritis, may lead to directly observed macrophage resorption of tissue, including articular cartilage and bone.
In summary, numerous factors may lead to the clinically observable decline in the mechanical stability of implanted joints after 10 years, particularly in aging and in excessively active patients. These are usually associated with the development of a fibrous membrane, which may or may not contain histiocytes reacting to particulate debris. However, experimental evidence would indicate that macrophages and histiocytes join in the reactive process of metallic wear debris, and may in and of themselves stimulate an ongoing inflammatory reaction in which numerous direct or indirect bone-resorbing and osteolytic materials, including cytokines, PGE2, and collagenase, may be released. This inflammatory reaction may be dramatic, with marked osteolysis and pseudogranulomatous tumors mimicking true tumors (Figs. 17.3A and 17.4B).
Implant Materials
A broad range of materials have been used in joint arthroplasties (Fig. 17.8) (Table 17.5). These include most notably:
Stainless steel (mostly iron with chromium, nickel, and molybdenum)
In the United States in 2012, 93 percent of THA were cementless, with 56 percent of THA bearings being metal highly cross-linked polyethylene (HXLPE) and 39 percent being ceramic-HXPLE. Ninety-nine percent of acetabular cups were modular. In regard to the femoral heads, 61 percent were metal and 39 percent were ceramic, and 51 percent were 36 mm and 28 percent were 32 mm. THA implant usage in the United States tends to favor cementless fixation using modular acetabular cups and large-diameter femoral heads with metal-on-polyethylene or ceramic-on-polyethylene bearings.
Interestingly, the majority of THR femoral stems are cementless in the United States, as opposed to many European countries. In Sweden, with a long-standing tradition of arthroplasty registries to record complications, the majority are cemented.
The stainless steel implant is usually made of an iron-based alloy that contains an array of elements, including iron, chromium, and nickel, often with added substances such as manganese, carbon, molybdenum, and silicone. The cobalt-chromium alloys are similarly complex mixtures of substances. Although the percentage of potentially toxic or even carcinogenic substances within these alloys is small, toxicity has been demonstrated with metals such as chromium and vanadium, and hypersensitivity with cobalt and nickel. One type of titanium contains aluminum, which in excess is known to be associated with several diseases (57).
FIGURE 17.6. Radiolucent lines. (A) A radiograph showing a radiolucent line under a wedge augment after conversion of a failed unicompartmental knee arthroplasty to a total knee replacement. (Reprinted with permission from Springer BD, Scott RD, Thornhill JS. Conversion of failed unicompartmental knee arthroplasty to TKR. Clin Orthop. 2006;446:214-220.) (B) Roentgenograph shows a radiolucent zone along the implant-bone interface in the tibia in a failed knee replacement. (C) Radiolucent line along femoral stem (yellow arrows).
FIGURE 17.7. Grossly, a loosened polyethylene tibial component is seen and thickened fibrous membrane.
In addition to various metals, implanted devices in orthopaedic arthroplasty include plastic components such as the PE acetabular cup often used in hip replacements. The traditional fixation device is a PMMA polymer (or bone cement). All these substances have been associated with documented tissue reactions in human implants. Although some of the debrided material may be seen on routine histologic preparations, in most cases the particulate matter in failed prostheses is too small to be detected under light microscopy.
An interesting complication associated with ceramic on ceramic implants is actually audible. “Squeaking” has been most intensely studied, but clicking, snapping, and grinding can also occur (58). Thought to involve 0.5 to 20 percent of ceramic on ceramic implants, a likely cause is edge loading. Squeaking may also be related to impingement, component malposition, separation between liner and shell, and third-body noise.
Metals
The most commonly used metal implants in the United States for hip and knee replacements are carbon stainless steels, titanium, and cobalt-chromium alloys (59). Stainless steels and cobalt-chromium implants contain nickel and molybdenum. Other alloys used are vanadium and aluminum.
Inflammation-mediated changes are complex and result in the production within tissue around the prosthesis of numerous factors, including IL-1 and IL-6, TNFα, and the osteoclastogenic molecules, RANK and RANKL (60). The macrophage is the primary cell mediator (61,62) (Fig. 17.4).
It can be assumed that with orthopaedic implants, metal ions will leak out into the tissue and synovial fluid (59). To what extent this has a negative effect depends in part on the degree of leakage, the ability to generate an inflammatory reaction, and in some circumstances, the development of an allergy to the corrosively produced metal ions. When skin testing is performed, the incidence of allergy to metal has been estimated to be about 15 percent by Merritt (63). The incidence of allergies such as to cobalt has been estimated to be 28 percent by Elves et al. (64). Nickel, which has been shown to be released from stainless steel prostheses in experimental models, is known to be associated with urticarial and eczematous dermatitides (65). In fact, it ranks third among the five most common causes of allergic contact dermatitis (66). Although it is possible that these reactions may contribute to bone pathology or loosening of the prosthesis (67), adverse effects in tissue have not been well documented, and more significant systemic effects have been less well established.
In both early and late studies of the McKee-Farrar type of total hip prosthesis, the prostheses appear dulled, with microscopic evidence of abrasive scratch marks (68). These scratches were associated with wear particles, readily found in both the joint fluid (Fig. 17.9) and the tissue around the prosthesis. This type of metal-on-metal debridement can lead to a grayish black discoloration that is apparent on gross examination of involved tissue (69,70) (Fig. 17.9). Black pigmentation is due to metal oxides that form on the surface of chromium-cobalt or titanium alloys due to an electrolytic process. The metal particles are round or rodlike, 1 to 2 µm in size, and readily viewable on polarized light microscopy. They are present extracellularly and intracellularly within both histiocytes and fibroblasts. Giant cell reactions to metallic debris are less common than to cement and PE.
Implants of titanium alloy are more likely to generate wear debris, and therefore inflammatory mediators are implicated in osteolysis more frequently than with implants of cobalt-chrome alloys (71). Cobalt-chromium particles are likely to be more toxic (72). Clinical studies have documented a pattern of increased metal content in serum, urine, and tissue evaluated following soft tissue implants, segmental bone replacements, and joint arthroplasties. Metal-on-metal implants have been shown to have 7 times more erythrocyte cobalt levels, 41 times more urine cobalt levels, and 14 times more urine chromium levels than that observed in metal on PE-bearing surfaces (73). Similar studies suggest that long-term exposure to systemic metal ion should be a matter of cautious concern (74). Corrosion rates for various metals and alloys have been estimated.
Metal hip joints release particles at an annual wear rate calculated to be an average of approximately 5 mm3, considered low compared with the rate for PE (75). This, coupled with the small size of metal particles, corresponds on light microscopy to a less intense granulomatous and foreign body giant cell reaction (76) (Table 17.6). Grossly, tissue retrieved from failed titanium metal-on-metal implants is grayish or black, whereas that from failed metal-on-PE implants is somewhat orange or tan.
Although most of the released metals, except titanium, have defined pathophysiologic roles in human metabolic cycles, some, such as aluminum, can be frankly toxic. Widespread dissemination of metal debris from implants has been associated with necrobiosis (76).
The mechanism for the production of implant debris most probably starts at the ion level. Collier et al. (77) have described corrosion as involving the dissolution of the metal alloy into its respective ions. Subsequent reduction of oxygen to hydroxide ions produces an excess of positive charge, initiating a destructive ionic exchange.
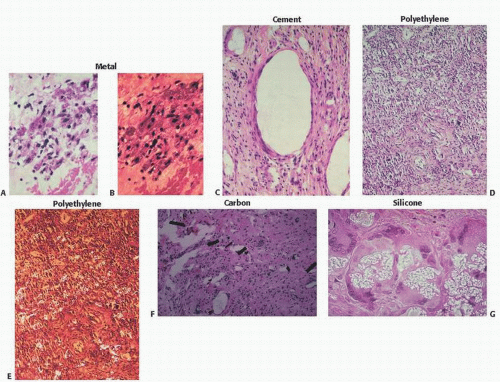
FIGURE 17.8. Implant materials at a glance. (Also see Table 17.5.) Metal (A), light microscopy; (B), polarized light microscopy); cement (C), polyethylene (D), light microscopy; (E), polarized light microscopy); carbon (F), and silicone (G).
Clearly, the cellular reaction to metal debris involves in part immunologic mediators such as lymphocytes, but most conspicuously, cells of histiocyte/macrophage lineage. In describing a sinus histiocytosis of pelvic lymph nodes following hip replacement, Albores-Saavedra et al. (78) demonstrated metal and PE in the nodes, and the histiocyte lineage of the phagocytosing cells was confirmed by immunoreactivity for classic histiocyte markers (lysozyme, α1-antitrypsin, α1-antichymotrypsin, and cathepsin D). The cell-mediated release of cytokines as a cause of bone resorption and osteolysis is well established in PE models (79,80). Metal debris from implants has been documented at distant sites (81) and in regional lymph nodes (82).
Although oncogenic effects will be discussed in greater detail later, there is abundant evidence that nickel, cobalt, and chromium have an oncogenic effect in animals. Stainless steel internal fixation devices are known causative agents of tumors in animals (83).
Metal-on-Metal Arthroplasties
In recent years, adverse tissue reactions and potential adverse clinical events associated with the use of metal-on-metal prostheses have been increasingly documented, leading to caution in their use. In 2013, the United Kingdom announced a ban on their use in National Health Service hospitals, and in the United States, they were recalled by manufacturers.
How did this come about? Hip prostheses utilizing a metal ball in a metal socket (MoM) were widely used in the 1960s, but the observation of black staining of periarticular tissues by metal debris led to a shift in the use of polyethylene sockets (26). Subsequent association of osteolysis associated with polyethylene wear debris revived interest in MoM. Although early clinical results were acclaimed favorable by some, increasing failure rates at early stages of implantation were initially anecdotally reported, but subsequently well documented in arthroplasty registries.
Radiographic analyses, histologic analyses, and serum investigations have led to documentation of a range of adverse reactions (Fig. 17.10) and a plethora of terms to categorize them including:
ALTR—adverse local tissue reactions,
ARMD—adverse reaction to metal debris,
Metallosis—the presence of grossly observable grayish-black tissue staining and/or identification of metal particles on histologic examination and/or circulating metal ion levels,
Pseudotumor—the presence on imaging or observation during surgery or histologic examination of solid or cystic masses in close proximity to the arthroplasty site,