and Aysegul A. Sahin2
(1)
Division of Pathology, Singapore General Hospital, Singapore, Singapore
(2)
The University of Texas, M. D. Anderson Cancer Center, Houston, TX, USA
Keywords
DuctalHistologic gradeSpecial typesTriple-negativeTumour-infiltrating lymphocytesMetaplasticMost breast malignancies arise from epithelial cells of terminal ductal lobular units and are categorised as carcinomas [1–3]. Invasive or infiltrative carcinoma refers to a proliferation of neoplastic cells with penetration through the basement membrane of ducts and lobular units into the breast stroma. Breast carcinoma, although often discussed as a single disease, actually constitutes a diverse group of tumours that differ in clinical presentation, imaging features, histopathologic appearance, expression of biologic markers, and clinical behaviour. Several histological subtypes of invasive breast carcinoma have been recognised based on a wide range of criteria, including cell type, architectural features, type and location of secretions, and biomarker profiles. The WHO classification of breast tumours recognises 21 different histologic types of breast cancer with distinct morphologic features [1]:
Invasive ductal carcinoma (invasive carcinoma no special type, invasive carcinoma not otherwise specified)
Invasive lobular carcinoma
Tubular carcinoma
Invasive cribriform carcinoma
Mucinous carcinoma
Carcinoma with medullary features
Carcinoma with apocrine differentiation
Carcinoma with signet-ring cell differentiation
Invasive micropapillary carcinoma
Metaplastic carcinoma
Carcinoma with neuroendocrine features
Secretory carcinoma
Invasive papillary carcinoma
Acinic cell carcinoma
Mucoepidermoid carcinoma
Polymorphous carcinoma
Oncocytic carcinoma
Lipid-rich carcinoma
Glycogen-rich clear-cell carcinoma
Sebaceous carcinoma
Salivary gland/skin adnexal-type tumours
Invasive breast cancers are broadly classified into invasive carcinomas with special morphologic types and invasive carcinomas without any special morphologic features. When an invasive carcinoma does not have any special histologic features, the terms invasive or infiltrative ductal carcinoma, invasive carcinoma no special type, or invasive carcinoma not otherwise specified are used. Some special types of breast carcinomas have relevant prognostic implications, and it is clinically important to recognise them. Others have unique morphologic features but have no special biologic behaviour associated with the special morphology. Mucinous carcinoma is described in Chap. 6; invasive lobular carcinoma is detailed in Chap. 10; invasive papillary and micropapillary carcinomas are included in Chap. 4. Some of the vanishingly rare subtypes are not specifically described.
Invasive Ductal Carcinoma (Invasive Carcinoma No Special Type, Invasive Carcinoma Not Otherwise Specified)
Definition
Invasive ductal carcinoma or infiltrative ductal carcinoma is defined as an invasive breast cancer with histologic features that do not fit any of the special types of breast cancer. Therefore, the diagnosis of invasive ductal carcinoma is based on the exclusion of other special types of breast cancers [1–3].
Clinical and Epidemiological Features
Invasive ductal carcinoma constitutes 45–75 % of all invasive breast carcinomas and comprises a heterogeneous group of tumours. The main reason for the wide incidence range reported in the literature is that many breast cancers show focal components of special types of breast carcinoma [4–7]. Many invasive carcinomas show a mixture of growth patterns, and some experts recognise a mixed invasive ductal and special-type carcinoma category. The amount of special-type carcinoma that is required for a tumour to be categorised into a mixed category is not well established in the literature. For tumours with excellent prognosis, such as tubular carcinoma or invasive cribriform carcinoma, more than 90 % of the tumour must be special type in order to classify it as such. In the case of other types of special carcinomas, however, there are no established criteria for designating a tumour as a mixed category or simply classifying it as an invasive ductal carcinoma. The term “ductal” does not imply that these tumours arise from ducts; rather, it indicates that these tumours commonly show ductal differentiation.
There are no specific clinical features that distinguish invasive carcinoma of no special type from other types of invasive breast cancer. Invasive ductal carcinoma occurs in a wide age range [1]. Although it can occur at any age, it is more common in the fifth and sixth decades. In most series, the average age is 55–60 years. The incidence decreases after age 80. A painless, palpable mass is the most common presentation. Nipple discharge or retraction, skin fixation, or oedema can be seen in advanced cases. Some patients present with redness of the breast skin (inflammatory breast carcinoma) (Fig. 12.1). The average tumour size at the time of diagnosis is about 2 cm. Patients diagnosed from screening mammography tend to have smaller lesions [8].

Fig. 12.1
Inflammatory breast carcinoma shows reddened skin over the breast, which may feel warm. Histologically, it corresponds to the presence of dermal lymphovascular emboli (Courtesy of Dr. Benita Tan)
Imaging Features
Invasive ductal carcinomas most commonly present as masses on radiology. Because of its infiltrative growth pattern, it usually appears irregular and lobulated on mammography, in contrast to benign mass-forming lesions, which tend to be round or oval (Fig. 12.2). Margins of the mass are typically irregular, with spiculated borders corresponding to an invasive growth pattern on histologic evaluation (Fig. 12.3). Microcalcifications (grouped, clustered, or segmental in appearance) are commonly found on mammography (Fig. 12.4). Microcalcifications are more frequently associated with the in situ carcinoma component of the tumour, though the stroma of invasive carcinoma or necrosis within the invasive carcinoma can also show microcalcifications. Ultrasound typically reveals an irregular mass with indistinct margins and inhomogeneous echo texture with acoustic shadowing (Fig. 12.5) [9]. On MRI, invasive carcinoma usually appears as an irregular mass with enhancement kinetics that show a suspicious rapid wash-in and wash-out pattern. Several other functional MRI techniques are also applied to improve the diagnostic evaluation.




Fig. 12.2
Invasive ductal carcinoma. Radiographic and gross features. (a) Mammogram shows a radiodense mass with irregular, infiltrating borders. (b) Mastectomy specimen shows a grey-white mass invading the fatty breast parenchyma
Fig. 12.3
Invasive ductal carcinoma. Gross and microscopic features. (a, b) Strands of grey-white tissue infiltrate the adipose tissue. (c, d) Histologic sections of the tumour show tumour cells growing into adipose tissue with associated fingerlike projections corresponding to the infiltrative gross appearance
Fig. 12.4
Invasive ductal carcinoma. Radiographic and gross features. (a) X-ray of an irregular tumour mass associated with a large area of microcalcifications. (b) Corresponding irregular grey-white mass with white, fibrous streaks indicating tumour extension
Fig. 12.5
Invasive ductal carcinoma. Sonographic and gross features. (a) Tumour appears as a hypoechoic mass with posterior shadowing. (b) Corresponding excised specimen shows an irregular mass
Pathologic Features
Macroscopic Pathology
Most invasive ductal carcinomas form solid masses with ill-defined margins and infiltrative edges (Fig. 12.6) or are round and circumscribed with pushing margins (Fig. 12.7). Some tumours have contours with a mixture of these patterns (Fig. 12.8). The consistency and colour of the lesion vary based on the amount of stroma present within the tumour. Invasive carcinomas with an abundant stromal component appear more grey-white and tend to be firm on palpation. In contrast, tumours with less stroma appear tan or yellow and are softer (Fig. 12.9). Certain tumours appear red-brown, not only because of dense cellularity but also because of other morphologic features such as papillary growth pattern and intratumoural haemorrhage (Fig. 12.10). These tumours typically have a concave cut surface as a distinguishing feature, in contrast to benign lesions such as fibroadenomas, which have convex, bulging cut sections (Fig. 12.11). Cystic change can rarely be present and is usually due to tumour necrosis (Figs. 12.12 and 12.13).
Because the tumour size is an important prognostic factor of breast cancer, macroscopic evaluation of tumour size is essential, with careful measurement expressed in three dimensions. Dimensions of smaller tumours are confirmed microscopically. Satellite tumour nodules may be present (Fig. 12.14).









Fig. 12.6
Invasive ductal carcinoma. Gross features. (a–c) Different examples of invasive ductal carcinoma showing typical infiltrative margins
Fig. 12.7
Invasive ductal carcinoma. Gross features. (a–c) Tumour examples presenting with well-defined margins and pushing edges
Fig. 12.8
Invasive ductal carcinoma. Gross features. (a, b) Examples showing both well-circumscribed (arrow) and infiltrative (opposite side) growth patterns in the same tumour
Fig. 12.9
Invasive ductal carcinoma. Gross features. (a) The white appearance of this tumour is due to extensive stromal fibrosis. (b) The grey-tan appearance of this large invasive tumour is due to high tumour cellularity and scant stroma. (c) Close-up of the tumour in (b) shows a white area indicating abundant stromal fibrosis (arrow) in a background of nodular tumour growth
Fig. 12.10
Invasive ductal carcinoma. Gross features. (a) Invasive carcinoma with high tumour cellularity on histology, shows prominent papillary growth and a red-brown appearance. (b) Higher magnification of (a). (c) The red-brown colour of this intracystic tumour is due to intratumoural haemorrhage
Fig. 12.11
Comparison of gross features of invasive ductal carcinoma and fibroadenoma. (a) Cut section of invasive ductal carcinoma is typically concave with central indentation. Yellow-white fibrous strands extending into and retracting the surrounding tissue result in a concave appearance with central indentation (arrow). (b) In contrast, the cut section of a fibroadenoma is bulging
Fig. 12.12
Invasive ductal carcinoma. Gross features. Example of tumour with areas of haemorrhage and necrosis leading to cystic spaces (arrows)
Fig. 12.13
Invasive ductal carcinoma. Radiographic and gross features. (a) X-ray of invasive ductal carcinoma in a section of a total mastectomy and its corresponding gross specimen showing an irregular grey-white mass replacing almost the entire breast parenchyma, involving the subareolar region. (b) Higher magnification shows a nodular growth pattern with areas of punctate necrosis (arrows)
Fig. 12.14
Invasive ductal carcinoma. Gross features. (a, b) Invasive ductal carcinoma with satellite nodules (arrows)
Microscopic Pathology
The microscopic appearance of invasive ductal carcinoma is highly variable [1–3]. The degree of tumour cellularity, growth pattern, extent of associated in situ carcinoma component, degree of cytologic atypia, mitotic activity, amount of stroma, presence or absence of necrosis, and the presence and amount of lymphocytic infiltrate in the stroma and among tumour cells all vary significantly in different tumours. Some of these features may even differ in different areas of the same tumour [10–13]. Tumour cells may show varying degrees of gland formation (Fig. 12.15); may form nests, cords, or trabeculae; or may grow in solid sheets. Necrosis may be present and can be extensive, potentially leading to pseudocyst formation. The appearance of malignant cells varies significantly. Some tumours have minimal cellular atypia and pleomorphism; the tumour cells are small and uniform, similar to the cells of normal duct epithelium. In other tumours, there can be marked cellular atypia and pleomorphism, with tumour cells that have enlarged, hyperchromatic nuclei (Fig. 12.16). The degree of mitotic activity varies significantly, from abundant and easily identified to almost none. Focal mucin production (both intracellular and extracellular) can sometimes be seen. Squamoid, clear-cell, and apocrine differentiation are other histologic findings that can be observed. Similar to tumour cells, the stroma may display marked variation in its amount, composition, and distribution. The amount of stroma can range from none to abundant (Fig. 12.17). Some tumours have large amounts of dense, hyalinised stroma resulting in a very firm consistency, termed scirrhous carcinoma. In some tumours, the stroma consists of only collagen, whereas others are cellular and include fibroblasts and myofibroblasts (Fig. 12.18). Elastosis can be present. Stromal distribution throughout the tumour is also variable. Tumour cells may proliferate around the central sclerotic stromal component, but in other tumours, the stroma is uniformly distributed (Figs. 12.19 and 12.20). Calcifications can be detected in more than half of the cases. Additionally, the amount of lymphoplasmacytic infiltrate in tumour and stroma varies considerably, from moderate or marked to none (Fig. 12.21). Recent studies have suggested that the amount of lymphoplasmacytic infiltrate may have a prognostic and potentially predictive value, particularly in triple-negative and c-erbB-2-overexpressing breast cancers [14]. Osteoclast-like giant cells or giant-cell granulomas are rarely seen in the stroma. With adequate sampling of the tumour, an in situ carcinoma component can be identified in most cases of invasive ductal carcinomas (Fig. 12.22). The in situ component is most often ductal, but rarely it can be lobular. When ductal carcinoma in situ (DCIS) is identified, its grade is usually similar to that of the invasive component. The presence of lymphovascular invasion should be carefully evaluated in all invasive ductal carcinomas, preferably at the peripheral aspect of the tumour (Fig. 12.23) [15, 16]. Retraction artefacts that are commonly seen around clusters of tumour should not be confused with true lymphovascular space invasion. Unless a tumour embolus is identified in a large blood vessel, it is not recommended to try to distinguish small capillaries from lymphatics. Perineural invasion occasionally may be seen, but this finding is not of prognostic significance (Fig. 12.24) [17].










Fig. 12.15
Invasive ductal carcinoma. Microscopic features. Three different invasive ductal carcinoma cases show more than 75 % glandular differentiation (a) compared with 30 % (b) and less than 10 % (c)
Fig. 12.16
Invasive ductal carcinoma. Microscopic features. (a) Low-grade tumour composed of uniform tumour cells having small nuclei, which are similar to adjacent normal ductal cells. (b) High-grade tumour with a solid growth pattern and moderate to marked nuclear atypia characterized by significant variation in nuclear size and shape
Fig. 12.17
Invasive ductal carcinoma. Microscopic features. (a) Invasive carcinoma with minimal stromal component. (b) Tumour showing a moderate amount of stroma. (c) Invasive tumour with abundant, fibrous, collagenised stroma
Fig. 12.18
Invasive ductal carcinoma. Microscopic features. (a) The stroma of this invasive tumour consists predominantly of collagen bundles without a cellular component. (b) Highly cellular stroma, in contrast to (a)
Fig. 12.19
Invasive ductal carcinoma. Microscopic features. (a) Low magnification of the tumour, showing a central, sclerotic area with tumour cells radiating outwards. (b) Medium magnification of the periphery of the same tumour. (c) High magnification of tumour in the sclerotic centre
Fig. 12.20
Invasive ductal carcinoma. Microscopic features. Uniform distribution of sclerosis, unlike Fig. 12.19
Fig. 12.21
Invasive ductal carcinoma. Microscopic features. (a) Invasive carcinoma with no tumour-infiltrating lymphocytes. (b) Invasive carcinoma with extensive lymphocyte infiltration. (c) Higher magnification of (b)
Fig. 12.22
Invasive ductal carcinoma. Microscopic features. Invasive carcinoma with associated in situ ductal carcinoma component (right lower field). The nuclear grade is similar in both components though this may be difficult to appreciate at this magnification
Fig. 12.23
Invasive ductal carcinoma. Microscopic features. (a) Lymphovascular space invasion of ductal carcinoma. Clusters of carcinoma cells are seen in endothelium-lined spaces away from the invasive carcinoma. (b) Higher magnification shows the flattened endothelial cells lining the spaces (arrows)
Fig. 12.24
Invasive ductal carcinoma. Microscopic features. Lower (a) and higher (b) magnification of invasive carcinoma showing perineural invasion. Lower (c) and higher (d) magnification of another example of perineural invasion. Note that the malignant glands surround and indent the nerve
Grading of Invasive Ductal Carcinoma
Grading of invasive ductal carcinoma of the breast has been shown to be a robust predictor of clinical outcome [18–24]. Providing a grade for all newly diagnosed breast cancers has been recommended by several different breast cancer practice guidelines, including the College of American Pathologists (CAP), American Society of Clinical Oncology (ASCO) and the American Joint Committee on Cancer (AJCC). Several different grading systems using either nuclear features, architectural growth pattern, or a combination of these have been proposed [18, 21, 24]. The most widely used grading system is the Nottingham histologic grading, which was modified by Elston and Ellis [18] to include precise definitions. In this grading system, three tumour characteristics—tubule formation, nuclear pleomorphism, and mitotic count—are evaluated using defined criteria (Table 12.1). Each characteristic is assessed separately and given a score of 1–3, with the values being added to reach a final score of 3–9. Final grading is assigned based on this score, as shown in Table 12.2. The relative importance of the components of this grading system is uncertain, but it is essential to apply the histologic criteria strictly. The subjective nature of histologic grading and interobserver agreement rates have been extensively studied in the literature [19, 20]. Technical factors such as quality of tissue fixation, preservation, and section preparation are recognised as some of the main problems that contribute to poor interobserver reproducibility. Therefore, the well-defined guidelines recommended by the College of American Pathologists for tissue handling should be followed.
Several studies have evaluated the concordance rates of breast cancer grading on core needle biopsy and excision [25, 26]. Most studies show good concordance when there is adequate tumour on core needle biopsy. Tumour heterogeneity is a main concern when determining the grade of breast cancer on small samples. Reported studies suggest that a histologic grade can be reliably assessed from core needle biopsies in most cases. In clinical practice, the core needle biopsy specimen will be the only sample available for patients who are undergoing neoadjuvant therapies. Recent molecular studies emphasise the importance of histologic grading, as breast cancers with different grades show distinct molecular profiles at genomic, transcriptomic, and proteomic levels [13, 21].
Table 12.1
Grading of invasive ductal carcinoma
Score | 1 | 2 | 3 |
|---|---|---|---|
Tubule formation | >75 % | 10–75 % | <10 % |
 |  |  | |
Nuclear pleomorphism | Uniform | Moderate variation | Marked variation |
 |  |  | |
Mitotic count* | Rare | Occasional | Abundant |
 |  |  |
Table 12.2
Histological grade scoring
Grade | Summary score |
|---|---|
Grade 1 (well differentiated) | 3–5 |
Grade 2 (moderately differentiated) | 6–7 |
Grade 3 (poorly differentiated) | 8–9 |
Immunohistochemistry Features
Invasive ductal carcinoma cells are typically positive for cytokeratin 7. Luminal type cytokeratins (cytokeratin 7/8, 18, and 19) are positive in most tumours, whereas basal cytokeratins (cytokeratin 5/6 and 14) are positive in only a small subset of breast carcinomas. Nearly all invasive ductal carcinomas are negative for cytokeratin 20, and they are positive for epithelial membrane antigen and E-cadherin. Gross cystic disease fluid protein 15 (GCDFP-15) and mammaglobin are reported to be positive in 50–70 % of invasive ductal carcinomas [27, 28]. GATA3 expression is closely related to the molecular typing of breast cancer, and it is present in 90 % of invasive ductal carcinomas. It is expressed in almost 100 % of oestrogen-positive tumours, although at lower levels in oestrogen receptor-negative and triple-negative breast cancers (Fig. 12.25) [29]. Similarly, FOXA1, a member of the forkhead transcription factor family, is associated with oestrogen receptor expression. Studies have shown that FOXA1 is an excellent breast carcinoma marker, but its utility is limited in the triple-negative subtype [30]. Two thirds of invasive ductal breast carcinomas are positive for oestrogen and progesterone receptors. In addition to being prognostic markers, these receptors also predict the likelihood of response to endocrine therapy [31]. In current clinical practice, about 15 %–20 % of invasive ductal carcinomas show c-erbB-2 (HER2/neu) protein overexpression or gene amplification, correlating with high-grade carcinomas (Fig. 12.26). The primary clinical use of c-erbB-2 is to predict the likelihood of response to c-erbB-2-targeted therapy [32].


Fig. 12.25
Invasive ductal carcinoma. Immunohistochemical features. Strong positivity for oestrogen receptor in a low-grade invasive ductal carcinoma (a). Diffuse positivity for GATA-3 (b) in the same tumour. High-grade invasive carcinoma (c). The same case shown in (c) is negative for oestrogen receptor (d) and focally positive for GATA-3 (e) and gross cystic disease fluid protein 15 (f)
Fig. 12.26
Invasive ductal carcinoma. Immunohistochemical features. (a) H&E section of a (poorly differentiated) invasive ductal carcinoma. (b) Invasive carcinoma shows strong (3+) membrane staining for c-erbB-2. (c) Corresponding fluorescence in situ hybridisation shows increased c-erbB-2 gene copy number (red signals represent the number of c-erbB-2 gene copies and green signals correspond to CEP17)
Molecular Classification
Over the past two decades, the advent of genomic technologies has allowed molecular characterisation of breast cancer and supported the concept that invasive ductal carcinoma is not a single tumour type but a collection of biologically and clinically different tumours arising from the breast epithelium. Based on high-throughput gene expression analysis, four different molecular types of breast carcinoma were originally described: luminal A, luminal B, basal-like, and c-erbB-2 positive [33–36]. Recent studies have identified several additional distinct subtypes of breast carcinomas, including claudin low, interferon rich, and molecular apocrine. Furthermore, six subtypes of basal-like carcinoma (basal-like1, basal-like2, immunomodulatory, luminal androgen receptor, mesenchymal-like, and mesenchymal stem-like) have been described. Multiple independent studies have demonstrated a significant association between these molecular classes of invasive ductal carcinomas and histologic grade, clinical behaviour, and response to systemic therapy [37–39]. Luminal A tumours account for 50 % of invasive breast cancers and generally correspond to low- to intermediate-grade, oestrogen receptor-positive, c-erbB-2-negative tumours with low proliferation. They include a wide range of low-grade invasive carcinomas, including classic lobular, tubular, and mucinous carcinomas. Luminal B tumours comprise 20 % of invasive breast cancers and correspond to intermediate- to high-grade, oestrogen receptor-positive tumours with a high proliferation rate; c-erbB-2 expression is variable (positive or negative) [36]. The c-erbB-2-positive molecular subclass includes generally high-grade carcinomas, which are mostly but not always c-erbB-2-positive by conventional immunohistochemical and gene amplification analyses. This group accounts for 15 % of all invasive breast cancers. They are usually negative for oestrogen and progesterone receptors, Ki-67 expression is high, and TP53 mutation is common. These tumours are more likely to have lymph node metastasis and poor prognosis. Basal-like carcinomas account for 15 % of all invasive carcinomas and include oestrogen receptor-negative and c-erbB-2-negative tumours; they are typically high-grade cancers with high proliferation rates. They express basal epithelial markers such as cytokeratins 5/6, 14, and 17. Subsets of these tumours also show mesenchymal differentiation as evidenced by spindle cell morphology and positivity for vimentin.
In clinical practice, immunohistochemical classification based on the expression of oestrogen and progesterone receptors, c-erbB-2 overexpression, and evaluation of proliferation markers is applied as a surrogate for molecular subtypes. Invasive ductal carcinomas are classified into four categories: oestrogen receptor-positive low proliferation, oestrogen receptor-positive high proliferation, c-erbB-2 positive, and triple-negative. These four categories roughly correspond to the molecular subtypes. The importance of these markers has been shown in multiple studies, and recently it has been proposed that these biomarkers should be included in the staging of breast cancer [40].
Differential Diagnosis
The differential diagnosis of invasive ductal carcinoma includes malignant tumours such as special types of invasive breast cancers, metastatic carcinomas, non-invasive carcinomas, and benign lesions such as sclerosing adenosis and radial scar.
Invasive ductal carcinoma should be distinguished from special types of invasive carcinomas, especially those associated with exceptionally favourable prognoses, including tubular, invasive cribriform, and mucinous carcinomas. Invasive ductal carcinoma with extensive tubule formation may mimic tubular carcinoma. The diagnosis of tubular carcinoma should be restricted to tumours that show tubule formation in more than 90 % of the tumour. In tubular carcinoma, tubules are lined by a single layer of low-grade tumour cells. In contrast, well-differentiated invasive ductal carcinomas with extensive tubular differentiation show tubules that are lined by more than one layer of cells which typically show nuclear atypia. Metastatic carcinomas may mimic invasive ductal carcinoma. The presence of DCIS is good evidence for establishing the diagnosis of primary breast cancer. It is important to remember that some metastatic tumours may show a nested growth pattern mimicking in situ ductal carcinoma. Clinical history and immunohistochemical stains can be used to establish the primary versus metastatic nature of the tumour.
In situ ductal carcinomas involving pre-existing lesions with infiltrative margins such as sclerosing adenosis may mimic invasive ductal carcinoma. This is a particularly major diagnostic pitfall when only a small biopsy sample is available. The demonstration of intact myoepithelial cells or intact basement membranes will establish the in situ nature of the ductal carcinoma. Similarly, benign lesions with infiltrative growth patterns may mimic invasive carcinoma (see Chap. 5).
Prognosis and Therapy Considerations
The prognosis for invasive ductal carcinoma depends on the stage of the disease and biomarker expression. Staging includes tumour size, lymph node status, and the presence or absence of distant metastasis. Therapy depends on the stage and involves a multimodality approach including surgery, radiation, and systemic therapy. Recently, targeted therapy and immunotherapy approaches have been integrated into clinical practice [41].
Invasive Breast Carcinoma, Special Types
Definition
Special types of breast carcinomas are defined based on specific morphologic features which may be associated with distinct biologic behaviour. These tumours collectively constitute approximately 25–30 % of all invasive breast cancers. Probably the most important special types of invasive carcinoma include tubular and invasive cribriform carcinomas, as well as mucinous carcinomas (see Chap. 6); these types are uniformly associated with good clinical outcomes [1, 2, 42].
Tubular Carcinoma
Definition
Tubular carcinoma is a well-differentiated invasive carcinoma composed almost completely of tubules, which are lined by a single layer of low-grade tumour cells and have open lumens.
Clinical and Epidemiological Features
Tubular carcinoma accounts for 2–10 % of all invasive breast cancers in published series. The wide range of reported incidence reflects variations of histologic criteria (percentage of tubules required) to establish this diagnosis and inclusion of patients’ data from screening programmes, in which the incidence of tubular carcinoma is much higher. Tubular carcinoma accounts for up to 25 % of carcinomas detected by mammographic screening, whereas it is less than 5 % of breast cancers in unscreened populations [43, 44].
Although tubular carcinoma has been reported in a wide age range (25–80 years), the average age is 60 years, which is slightly older than that of invasive ductal carcinoma. Most patients present with either a palpable mass or mammographic abnormality [44, 45]. Tubular carcinoma has also been documented in males. About 10–20 % of patients have been reported with multifocal tubular carcinomas growing as separate foci in one or more quadrants.
Imaging Features
Most tubular carcinomas present as irregularly shaped masses with spiculated margins and central density (Fig. 12.27a). In most cases, the spicules are longer than the diameter of the central lesion. Microcalcifications are present in half of the cases. Mammographic findings may overlap with radial scar. Sonography reveals ill-defined and hypoechoic masses, with posterior acoustic shadowing seen in the majority of cases [45].

Fig. 12.27
Tubular carcinoma. Radiographic, gross, and microscopic features. (a) Mammogram shows an irregular mass with spiculated margins (circled). (b) Excision of the same mass shows a grey-white tumour with irregular margins. (c) Microscopically, the same tumour is composed of well-formed tubules. (d) At higher magnification, it is seen that the tubules are lined by a single layer of cells having uniform morphologic features
Pathologic Features
Macroscopic Pathology
Most tubular carcinomas are less than 2 cm. Mammographically identified tumours tend to be less than 1 cm. They form grey-white, stellate nodules (Fig. 12.27b).
Microscopic Pathology
Microscopically, these tumours are characterised by a haphazard proliferation of angulated, oval, or elongated tubules with open lumens (Fig. 12.27c, d). The tubules have angulated contours with tapering ends and are lined by a single layer of epithelium without a peripheral myoepithelial cell layer (Fig. 12.28). The nuclear grade is generally low. However, focal nuclear atypia and enlargement (nuclear pleomorphism score of 2) may be allowed when tubular architecture is present throughout the tumour. The tumour cells have small nuclei, which resemble adjacent normal ductal epithelium. Individual tumour cells may form apical cytoplasmic snouts. Mitoses are very scant and difficult to find. The stroma can be fibrotic or elastotic. Infiltration of tubules into fat at the periphery of the tumour is commonly seen and is a helpful diagnostic clue in establishing the diagnosis. Concomitant occurrence of in situ carcinomas and epithelial proliferative breast lesions such as lobular neoplasia, flat epithelial atypia, and columnar cell change is common (Figs. 12.29 and 12.30) [46]. In almost all cases, the associated DCIS is low-grade and has cribriform or micropapillary patterns. Microcalcifications can be associated with either concomitant in situ carcinomas or epithelial proliferative lesions. Secretory material in neoplastic tubules can undergo calcifications.
When the tumour has areas of invasive lobular and tubular carcinoma in different proportions, it is referred to as tubulolobular carcinoma; multifocality is more frequent in tubulolobular carcinoma than in pure tubular carcinoma (Fig. 12.31) [47].
The percentage of the tubular carcinoma component that is required to designate a tumour as pure tubular carcinoma has been controversial in the literature. The WHO classification recommends that the diagnosis of tubular carcinoma is reserved for tumours showing more than 90 % tubule formation. Tumours showing 50–90 % tubular differentiation are classified as mixed, and those with less than 50 % are classified as invasive ductal carcinomas. Although the diagnosis of tubular carcinoma can be suggested from a needle core biopsy, the actual classification should be reserved to the final review of the entire lesion, to ensure that a non-tubular carcinoma component is not present. The great majority of tubular carcinomas are positive for oestrogen and progesterone receptors and negative for c-erbB-2 overexpression (luminal A type tumours) (Fig. 12.32).





Fig. 12.28
Tubular carcinoma. Microscopic features. (a) Low magnification of an infiltrative growth pattern having characteristic open tubules. (b) On medium magnification, some tubules show characteristic teardrop shapes. (c) High magnification shows apical snouts of the luminal aspects of some of the cells lining the tubules
Fig. 12.29
Tubular carcinoma. Microscopic features. (a) Low magnification of tubular carcinoma, showing an invasive growth pattern. The entire tumour displays tubular structures. (b) Higher magnification of the same tumour shows hypercellular stroma
Fig. 12.30
Tubular carcinoma. Microscopic features. The presence of premalignant/high-risk lesions is common adjacent to tubular carcinoma; columnar cell change and atypical ductal hyperplasia are seen here next to the tubular carcinoma
Fig. 12.31
Tubulolobular carcinoma. Microscopic features. This invasive carcinoma is composed predominantly of open tubules and focal, single-cell growth patterns
Fig. 12.32
Tubular carcinoma. Immunohistochemical features. Invasive carcinoma cells show diffuse strong positivity for oestrogen receptor (a) and progesterone receptor (b)
Differential Diagnosis
The differential diagnosis includes benign, small, glandular proliferations of the breast, and invasive carcinomas with tubular growth pattern. The absence of myoepithelial cells in tubules is the hallmark of tubular carcinoma, in contrast to benign small glandular proliferations (Fig. 12.33). Myoepithelial cells may be highlighted by immunohistochemical markers such as smooth muscle actin, smooth muscle myosin, or p63. (For detailed discussion, see Chap. 5). Microglandular adenosis is another benign lesion that may mimic tubular carcinoma (Fig. 12.34). Although the lack of a myoepithelial layer in microglandular adenosis glands is a major pitfall, their small and round shapes, in contrast to the angulated and irregular shapes of tubular carcinoma glands, are helpful in distinguishing the two entities. Cells lining microglandular adenosis glands are positive for S100 and negative for oestrogen and progesterone receptors and for epithelial membrane antigen (EMA); tubular carcinoma cells are almost always positive for hormone receptors and EMA. Other malignant tumours that mimic tubular carcinoma include well-differentiated invasive ductal carcinoma and low-grade adenosquamous carcinoma. Tubular carcinoma is not synonymous with invasive ductal carcinoma grade 1. Well-differentiated invasive ductal carcinomas have tubules lined by multiple cell layers, display areas of non-tubular growth pattern, and can have more nuclear atypia. Low-grade adenosquamous carcinoma may have well-formed tubules lined by low-grade tumour cells mimicking tubular carcinoma, but when sampled adequately, these tumours show solid nests and squamous differentiation even if they are focal. Adenosquamous carcinoma cells are typically negative for oestrogen and progesterone receptors; this negativity can assist in the differential diagnosis.


Fig. 12.33
Tubular carcinoma. Immunohistochemical features. (a) Immunohistochemical staining for p63. Tubular carcinoma glands lack staining, but entrapped normal ductal structures show strong positivity, indicating an intact myoepithelial layer in benign ducts. (b) Higher magnification of (a), showing detail
Fig. 12.34
Microglandular adenosis. Histologic features. Small glandular proliferation with an infiltrative pattern may mimic tubular carcinoma. Note the lack of cellular stroma and the round shape of glands, in contrast to the cellular stroma and angulated glands found in tubular carcinoma
Prognosis and Therapy Considerations
Tubular carcinoma generally has a low incidence of metastases to axillary lymph nodes and low recurrence rates, leading to a favourable prognosis [48, 49]. The prognosis of mixed tumours is worse than that of pure tubular carcinoma. The incidence of axillary metastases in tubular carcinoma ranges from 0 to 10 % in reported series, and the most important predictor of metastases is tumour size. In patients whose tubular carcinoma is less than 1 cm, the incidence of axillary metastasis is so low that some authors have suggested that axillary lymph node surgery can be omitted, but other authors have shown that axillary lymph node metastases can occur even with tumours less than 1 cm in size. In most cases, metastases also show a tubular carcinoma growth pattern, and only one to three lymph nodes are involved in almost all cases. The standard therapy protocol is segmental resection with sentinel lymph node dissection, followed by radiation therapy. Because the great majority of tubular carcinomas are positive for oestrogen and progesterone receptors, adjuvant hormonal therapy can be administered.
Invasive Cribriform Carcinoma
Definition
Invasive cribriform carcinoma is an invasive, well-differentiated carcinoma with a cribriform growth pattern similar to that of cribriform ductal carcinoma in situ (DCIS).
Clinical and Epidemiological Features
Invasive cribriform carcinoma is rare, representing 0.8–3.5 % of all invasive cancers. This tumour is closely related to tubular carcinoma, and a mixed tubular and invasive cribriform pattern is commonly seen. Because both tumours are associated with excellent prognosis, distinguishing these two components is less critical than verifying that invasive carcinoma not otherwise specified is not present [50]. To be designated as an invasive cribriform carcinoma, more than 90 % of the tumour must display a cribriform pattern. If an invasive carcinoma displays only tubules and cribriform islands, classification as either tubular or invasive cribriform carcinoma depends on which pattern predominates. Invasive cribriform carcinoma has been reported in a wide age range (20–90 years), with the average age in the mid-50s in most reported series [50, 51].
Imaging Features
Mammographic features of invasive cribriform carcinomas are similar to those of other invasive breast cancers. Most lesions present as spiculated masses, with or without microcalcifications. Not uncommonly, they can also present as fairly well-circumscribed masses with a regular shape. Multifocal tumours have been reported in up to 20 % of cases in some series.
Pathologic Features
Macroscopic Pathology
No specific macroscopic features associated with invasive cribriform carcinoma have been described. In most cases, lesions form stellate masses with infiltrative margins (Fig. 12.35).

Fig. 12.35
Invasive cribriform carcinoma. Gross features. (a, b) Tumour with infiltrative edges. Note the biopsy clip in the centre
Microscopic Pathology
Microscopically, invasive cribriform carcinoma is characterised by islands of uniform tumour cells with a cribriform appearance similar to that seen in cribriform DCIS. The tumour nests of invasive cribriform carcinoma usually have irregular borders and show clear-cut stromal invasion, in contrast to the rounded, smooth borders of in situ cribriform carcinoma (Figs. 12.36, 12.37, and 12.38). The nests of invasive cribriform carcinoma lack myoepithelial cells, the presence of which defines in situ cribriform carcinoma. Concomitant in situ carcinoma components, which frequently display cribriform patterns, are present in more than two thirds of the cases. Calcifications can be seen in neoplastic glands. Tumour cells are usually cuboidal to columnar, have low-grade to intermediate-grade nuclei, and typically have amphophilic cytoplasm. Minor areas of tubular differentiation are commonly seen. Mitotic figures are rare. The associated stroma usually appears cellular and reactive, which can be helpful in establishing the invasive nature, as in situ cribriform carcinomas usually do not have reactive-appearing stroma. Invasive cribriform carcinoma is the most common type of breast cancer associated with stromal or intraluminal osteoclast-like giant cells (Figs. 12.39 and 12.40). These cells have been described in many different histologic types of breast cancer and are thought to be histiocytic in origin, though they are not associated with a known biologic behaviour.
Similar to other well-differentiated breast cancers, invasive cribriform carcinomas are consistently positive for oestrogen and progesterone receptors and negative for c-erbB-2 overexpression (luminal A type tumours).





Fig. 12.36
Invasive cribriform carcinoma. Microscopic features. (a–d) Invasive carcinoma composed of cribriform structures with an infiltrative growth pattern. Low to high magnification of the same case
Fig. 12.37
Invasive cribriform carcinoma. Microscopic features. (a–d) Invasive carcinoma composed entirely of structures with a cribriform pattern. Low to high magnification of the same case
Fig. 12.38
Invasive cribriform carcinoma. Microscopic features. (a) Invasive carcinoma composed of large nests of uniform cells with cribriform patterns mimicking in situ cribriform carcinoma. The irregular, angulated edges of the nests indicate the invasive nature of the tumour. (b, c) Elongated cords and anastomosing islands of tumour cells show a cribriform growth pattern
Fig. 12.39
Invasive cribriform carcinoma with osteoclast-like giant cells. Invasive carcinoma comprising irregular cribriform glands is seen within the congested stroma. Scattered osteoclast-like giant cells (arrows) are seen among the invading cribriform islands. Cribriform ductal carcinoma in situ (DCIS) is present in the left upper field
Fig. 12.40
Invasive cribriform carcinoma with osteoclast-like giant cells. High magnification shows the osteoclast-like multinucleated giant cells (arrows) among the invasive cribriform islands
Differential Diagnosis
Invasive cribriform carcinoma should be differentiated from cribriform DCIS and other invasive carcinomas such as invasive ductal carcinoma and adenoid cystic carcinoma.
Although both in situ and invasive cribriform carcinomas have the same cribriform growth pattern, the nests of invasive cribriform carcinoma show more infiltrative edges. If the infiltrative edge is not present on a small biopsy specimen, the invasive nature of cribriform nests in invasive cribriform carcinoma can be confirmed by the absence of surrounding myoepithelial cells on immunohistochemistry. Invasive ductal carcinomas may have areas of cribriform growth pattern mimicking invasive cribriform carcinoma, but the tumour should almost totally show a cribriform pattern in order to be classified as invasive cribriform carcinoma.
Adenoid cystic carcinoma can be differentiated from invasive cribriform carcinoma on the basis of its typical dual cell proliferation (Fig. 12.41). Cribriform spaces of adenoid cystic carcinoma characteristically contain material resembling basement membrane, whereas spaces in invasive cribriform carcinoma are often empty. Furthermore, immunohistochemical staining for oestrogen and progesterone receptors will be helpful in this differential diagnosis. Adenoid cystic carcinomas are positive for cKIT and p63 and negative for oestrogen and progesterone receptors; invasive cribriform carcinomas are almost always positive for oestrogen receptor and negative for cKIT and p63 (Fig. 12.42) [52].
Collagenous spherulosis may superficially resemble invasive cribriform carcinoma, but this is usually a focal lesion with a lobulocentric growth pattern. Typically, the cribriform spaces contain basement membrane-like material (Fig. 12.43).



Fig. 12.41
Adenoid cystic carcinoma. Microscopic features. (a, b) The cribriform architectural pattern of adenoid cystic carcinoma may mimic invasive cribriform carcinoma. Adenoid cystic carcinoma glands contain basement membrane-like material, whereas cribriform carcinoma glands are usually empty
Fig. 12.42
Adenoid cystic carcinoma. Histologic and immunohistochemical features. (a, b) H&E staining of adenoid cystic carcinoma shows a cribriform pattern. (c) Tumour cells are diffusely positive for cKIT. (d) p63 staining highlights the presence of two cell populations in cribriform structures
Fig. 12.43
Collagenous spherulosis. Microscopic features. Lobulocentric proliferation of small glandular structures with a cribriform pattern, which may mimic invasive cribriform carcinoma
Prognosis and Therapy Considerations
The clinical behaviour of invasive cribriform carcinoma is very similar to that of tubular carcinoma, with a lower incidence of nodal metastases than for invasive ductal carcinoma [50]. Segmental resection with or without radiotherapy and sentinel lymph node sampling are considered standard treatment. Patients with small, pure invasive cribriform carcinomas have an excellent prognosis, and some authors question the need for radiation therapy after complete excision.
Carcinoma with Medullary Features
Definition
As the histological characteristics of classic medullary carcinoma are difficult to reproducibly define and recognise, the WHO Working Group recommends classifying these tumours as carcinomas with medullary features, a term that incorporates tumours previously categorised as medullary carcinoma, atypical medullary carcinoma, and invasive carcinoma with medullary features [53].
Clinical and Epidemiological Features
Classic medullary carcinomas account for less than 1 % of breast carcinomas. Studies that report higher rates likely included atypical forms and invasive carcinomas with medullary features. Patients tend to be younger and may present with palpable lumps. Some tumours are mammographically detected.
Imaging Features
These tumours are often circumscribed and may radiologically mimic a benign lesion (Fig. 12.44). Intralesional cystic components due to tumour necrosis may be seen.

Fig. 12.44
Atypical medullary carcinoma shows a circumscribed, lobulated mass on ultrasonography. This lesion was thought to be possibly a fibroadenoma radiologically (Courtesy of Dr. Lester Leong)
Pathologic Features
Macroscopic Pathology
Carcinomas with medullary features are macroscopically circumscribed, soft, fleshy tumours (Fig. 12.45). Cystic degeneration, necrosis, and haemorrhage may be seen (Figs. 12.46 and 12.47).



Fig. 12.45
Medullary carcinoma. Grossly, the tumour has circumscribed borders with a whitish cut surface. An area of haemorrhage is present in the central portion from prior needle aspiration
Fig. 12.46
Medullary carcinoma. This tumour has well-circumscribed but unencapsulated borders. There is a fleshy appearance with areas of haemorrhage and necrosis, the latter seen as yellowish foci in the tumour
Fig. 12.47
Atypical medullary carcinoma. Excision biopsy shows a soft, fleshy mass with lobulated contours and a rounded nubbin protruding against the adjacent fibrous breast parenchyma
Microscopic Pathology
The histological hallmark is the presence of a prominent lymphoplasmacytic infiltrate intermingling with high-grade carcinoma cells in a sheetlike growth pattern with little intervening stroma. Apart from the heavy lymphoplasmacytic infiltrate and high nuclear grade, classic medullary carcinoma shows microscopic circumscription, syncytial architecture in more than 75 % of the tumour, and absence of tubular differentiation. Mitoses, necrosis, and bizarre giant cells may be observed. In atypical medullary carcinoma (Figs. 12.48, 12.49, 12.50, 12.51, 12.52, 12.53, 12.54, 12.55, 12.56, and 12.57) and invasive carcinoma with medullary features (Figs. 12.58, 12.59, and 12.60), only some of these histological parameters are present. As there is interobserver inconsistency in defining the microscopic parameters, many (including the WHO Working Group) have opted for the encompassing diagnosis of carcinoma with medullary features. Receptors (ER, PR, c-erbB-2) are usually negative (“triple-negative”), and these tumours frequently show expression of basal markers and p53 (Figs. 12.61, 12.62, 12.63, and 12.64).





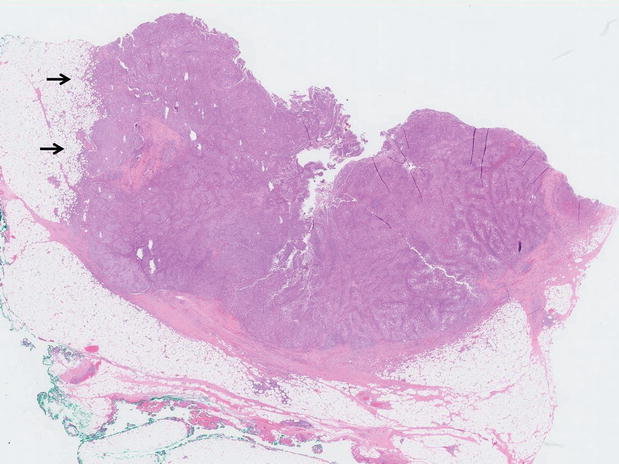








Fig. 12.48
Atypical medullary carcinoma. Scanning magnification shows a relatively circumscribed, lobulated tumour with pushing contours. The histological counterpart of the macroscopic tumour nubbin (Fig. 12.47) is observed protruding out into the surrounding breast parenchyma
Fig. 12.49
Atypical medullary carcinoma. Closer histological view of the rounded protrusion of the tumour, which has a cellular appearance with paler zones corresponding to the confluent sheets of malignant cells alternating with darker areas represented by the dense inflammatory cells
Fig. 12.50
Atypical medullary carcinoma. Broad, anastomosing trabeculae of tumour cells are seen among collections of lymphocytes
Fig. 12.51
Atypical medullary carcinoma. Bizarre and multinucleated tumour cells are seen among the sheets of malignant cells with markedly pleomorphic vesicular nuclei with prominent nucleoli. Some of the multinucleated tumour giant cells are reminiscent of syncytiotrophoblastic cells, but unlike syncytiotrophoblastic cells, these are negative for hCG and hPL
Fig. 12.52
Atypical medullary carcinoma. High magnification of the multinucleated giant cells intermingling with the carcinoma cells. A mitosis is present (arrow). Lymphocytes and plasma cells surround malignant cells, with some extending between them
Fig. 12.53
Atypical medullary carcinoma. Low magnification shows partial encapsulation with a fibrous wall, whereas part of the tumour reveals irregular extensions into the surrounding fat (arrows)
Fig. 12.54
Atypical medullary carcinoma. Some tumour cells show cytoplasmic vacuoles, which are likely degenerative in nature
Fig. 12.55
Atypical medullary carcinoma. At low magnification, a slight resemblance to a lymph node is seen. The tumour appears multinodular, with relatively good circumscription. No DCIS is present in the surrounding tissue. Though most medullary carcinomas are not accompanied by DCIS, and its presence is used by some authors as an exclusion criterion for the diagnosis of classic medullary carcinoma, it is possible for DCIS to be rarely encountered in association with medullary carcinoma
Fig. 12.56
Atypical medullary carcinoma. Syncytial sheets of high-grade carcinoma cells with atypical mitoses are accompanied by lymphoplasmacytic infiltrates within the tumour islands and in the intervening, scant stroma
Fig. 12.57
An axillary lymph node showing metastasis from an atypical medullary carcinoma. Anastomosing and coalescent tumour effaces a large portion of the node
Fig. 12.58
Invasive carcinoma with medullary features. This tumour has a lobulated outline with portions of the tumour extending into adipose. Lymphocytic infiltrates, though present, are less prominent, and there appears to be a greater amount of fibrosis meandering among the tumour islands
Fig. 12.59
Invasive carcinoma with medullary features. Islands of tumour cells are enveloped by lymphoplasmacytic infiltrates. The interphase between carcinoma islands and the stromal infiltrates is blurred, and many lymphocytes extend into the tumour as well
Fig. 12.60
Invasive carcinoma with medullary features. Lymphocytes are seen within the tumour islands (intratumoural lymphocytes), giving an appearance resembling lymphoepithelial carcinoma
Fig. 12.61
Medullary and medullary-like cancers are usually triple-negative. In this illustration, the tumour cells show negative staining for oestrogen receptor on immunohistochemistry. Note the internal positive control represented by the benign epithelial cell nuclei (arrow)




