Intraoperative Ultrasound of the Liver
Kristopher Croome
KMarie Reid Lombardo
INTRODUCTION
Intraoperative ultrasound (IOUS) of the liver involves the use of ultrasound imaging to provide real-time assessment during surgical procedures of the liver.1, 2, 3
In 1981, Makuuchi et al.4 described the use of IOUS (FIG 1) of the liver as an adjunct for hepatectomy; since then, the use of IOUS has expanded to include open percutaneous ablative techniques and various laparoscopic applications.
During laparoscopic surgery, where tactile examination is less feasible, IOUS can be extremely valuable during the exploratory phase of the operation. The following chapter provides a review on the technical aspects of IOUS of the liver.
The Physics behind Ultrasonography
Ultrasound measures the reflectivity of tissue to sound waves.
Amplitude is the maximum variation occurring in the sound wave (FIG 2).
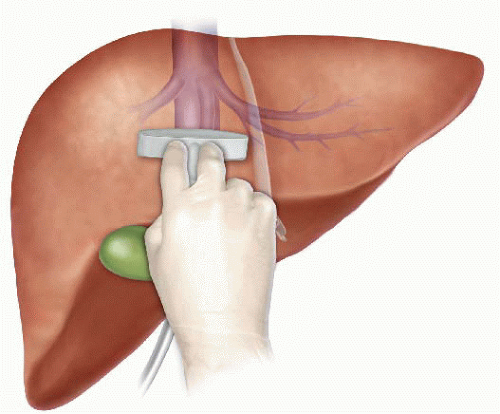
FIG 1 • IOUS with T-probe.
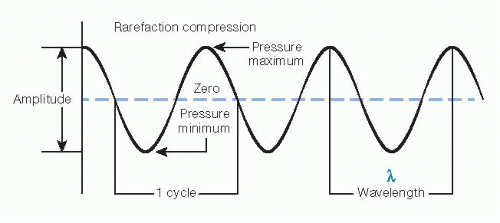
FIG 2 • Wave properties such as amplitude and wavelength.
Wavelength is the distance between the onset of peak compression or cycle to the next (FIG 2).
Velocity is the speed at which sound waves travel through a particular medium. Velocity is equal to the frequency × wavelength. Higher frequency will allow for greater penetration of the liver.
V=f×λ
Applications
IOUS has numerous applications with the goal of improving surgical decision making, guiding the operation, and thereby improving outcomes. Here are common examples of its use:
Evaluation of known hepatic lesions to determine the extent of known disease and scrutinize the proximity of lesions relative to major structures such as hepatic and portal veins. For primary liver tumors, this can be helpful in staging.
Detection of occult lesions not detected on preoperative imaging. Subcentimeter metastatic lesions may not be detected by preoperative computed tomography (CT) or magnetic resonance imaging (MRI). Their number and locations may alter surgical plan. IOUS has a reported sensitivity of 90% for the detection of hepatic lesions with positive and negative predictive values of 90% and 78%, respectively.2
Operative planning as resection planes may not follow anatomic segments and as such, it is important to delineate the mass and relationship to hepatic or biliary pedicles to ensure adequate hepatic vein and biliary drainage. IOUS has been shown to alter the operative plan, when that plan was based on preoperative imaging, in 17% to 44% of cases in several reports.2,5
Targeting of lesions for biopsy. If an unsuspected lesion is identified during surgery, IOUS-guided biopsy will help to determine the next steps.
Targeting of lesions for therapeutic ablation, microwave, or cryotherapy. Metastatic disease such as colorectal liver metastases may require a multimodality approach to treatment in order to achieve optimal control of disease.
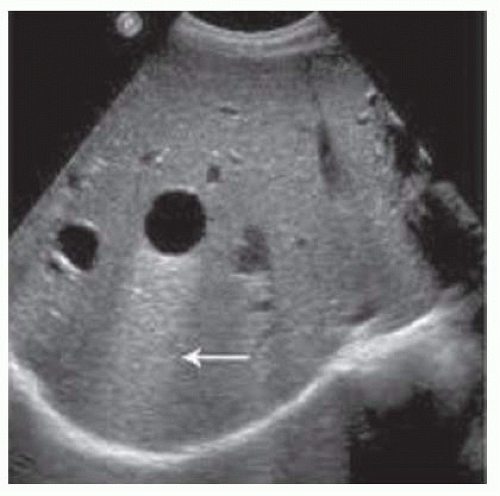 FIG 3 • Simple hepatic cyst with posterior acoustic enhancement (arrow). |
Liver Parenchyma
Normal liver parenchyma has a homogeneous echo pattern. Steatotic and cirrhotic livers have poor sound transmission and may appear diffusely hyperechoic.
Differential Diagnosis of Hepatic Lesions
If a lesion is encountered, it should be examined in both transverse and longitudinal directions to determine its full extent. Its proximity and extension to neighboring vessels should be determined.
Benign lesions
Cyst—The ultrasound appearance is a well-defined lesion, with very thin, almost unapparent walls, without circulatory signal at Doppler investigation. The content is transonic suggesting fluid composition (FIG 3).
Hemangioma—Hemangiomas frequently appear as well-circumscribed hyperechoic lesions with sizes of 2 to 3 cm. Doppler exploration reveals no circulatory signal, because although the lesions are highly vascular, the blood flow through them is relatively slow (FIG 4).
Adenoma—Adenomas can be very difficult to distinguish from other benign lesions such as focal nodular hyperplasia (FNH). The appearance of adenomas can range from hyper- to hypoechoic; however, they are most frequently hypoechoic (FIG 5).
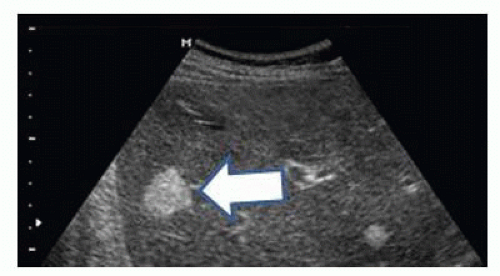
FIG 4 • Hemangioma (arrow).
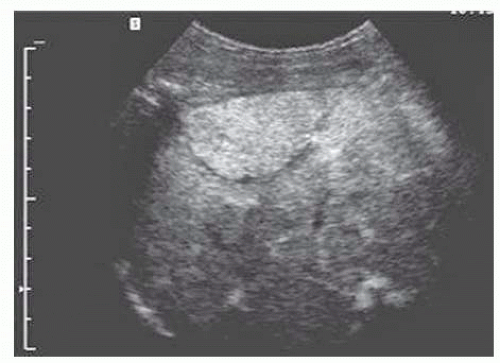
FIG 5 • Adenoma.
Neoplastic lesions
Hepatocellular carcinoma (HCC)—HCC appearance on 2-D ultrasound is that of an isoechoic or hypoechoic solid tumor, with imprecise delineation, with heterogeneous structure, uni- or multilocular (encephaloid form). HCC may also frequently invade portal and hepatic veins and so these should be examined particularly in larger tumors (FIG 6).
Colorectal liver metastases (CRLM)—CRLM usually appear hypoechoic. They may take on a “target” or “bull’s-eye” appearance due to alternating layers of hyper- and hypoechoic tissue. This pattern is highly suggestive of malignancy (FIG 7).
Neuroendocrine tumors (NETs)—Because NETs are hypervascular, they often appear as a hyperechoic lesion (FIG 8).
Required Equipment for Ultrasound
Liver IOUS is best performed using a real-time B-mode scanner system with a 5-MHz or 10-MHz side fire T-shaped linear array probe. Saline or conductive gel can be applied to the liver surface to augment wave transduction. Required components for IOUS include the following:
Transducer—Transducers help to transmit ultrasound waves through the hepatic parenchyma. There are a
variety of probes that are currently available and selection is based on the goal for the examination, body habitus and quality/character of hepatic parenchyma, and user preference. High-frequency probes allow for more adept superficial imaging, whereas lower frequency probes allow for deeper evaluation of the parenchyma. The most commonly used probe in open surgery is a T-probe. Probes can either be chemically sterilized or used with a sterile cover. Our group uses chemically sterilized probes (FIG 9).
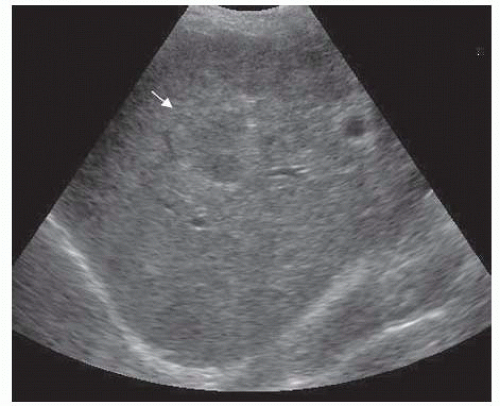
FIG 6 • HCC (arrow).
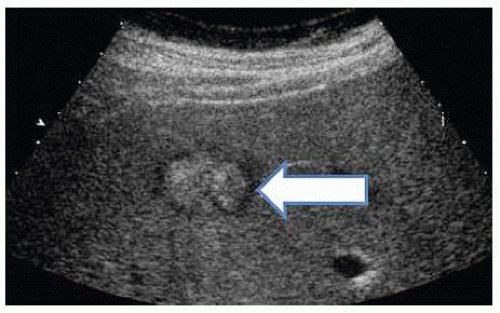
FIG 7 • CRLM showing peripheral rim or bull’s-eye appearance (arrow).
Processing unit: A variety of processing units are commercially available, most will include preset controls to adjust frequency, gain, depth, focus, freeze screens, and calipers to acquire measurements. We recommend familiarizing yourself with the processing unit available in your institution.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


