1 Inpatient medical care
Good medical practice
Providing good clinical care
The General Medical Council in the UK has published guidance for doctors and outlines their duties of care (www.gmc-uk.org). National practices differ from country to country but all have similar regulatory bodies and guidance. Remember:
Clinical records
Records should be written with a pen and be dated and signed, with a printed name below the signature. They must be legible, clear and accurate. They must include clinical findings, investigations and treatment(s) prescribed, the consent given, the decisions made and the information given to the patient, with details of follow-up or referrals. Records should be updated at the time of seeing the patient or soon after. The original record should never be altered but an additional note (signed and dated) should be made alongside any mistake. Records should be kept in a secure place. Computerized records are increasingly being used in some countries.
Assessment and general management
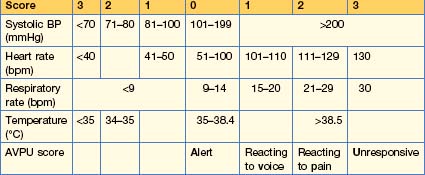
Modifed Early Warning Score (MEWS)
This simple physiological scoring system (Table 1.1) can be used at the bedside in a medical admission unit. It identifies patients at risk of deterioration who will require a higher level of care in either an HDU or an ICU.
SBAR
This is a mechanism by which teams can clarify what information should be communicated between members of the team. It develops better communication and teamwork, leading to increased patient safety. Standardized prompt questions in the four sections listed below are used to ensure that members of staff share concise and focused information with the correct level of detail. SBAR aids good communication and encourages prompt action on the part of the receiver.
• S Situation
• A Assessment
Pre- and peri-operative care and assessment
History and examination
Co-morbidities
Routine pre-operative tests
These are often not necessary in a patient undergoing minor or elective surgery.
Prophylaxis for deep vein thrombosis
Anti-DVT/VTE measures include early ambulation, which reduces the risk of DVT/PE. Graduated compression stockings (unless patient has peripheral arterial disease) and low-molecular-weight heparin or oral anti-thrombotic agents e.g. dabigatran or rivaroxaban should be used. See p. 245 for details.
Specific interviews
Breaking bad news
These interviews are often difficult. The aim is to make sure that the patient is enabled to understand and make the best of even very bad circumstances. These interviews should always be carried out in a quiet place and without interruption; if possible, patients should have someone with them. Explain your status and your responsibility to them.
Patient safety and infection control
Prescribing
The WHO Guide to Good Prescribing is a useful training programme to assist in prescribing medicines (http://whqlibdoc.who.int/hq/1994/WHO_DAP_94.11.pdf).
Drug metabolism
Pharmacokinetics (what the body does to the drug) and pharmacodynamics (what the drug does to the body)
Many drugs are metabolized by the liver. The metabolism varies between individuals, often because of changes in the cytochrome p450 family of enzymes. Inhibition or induction of cytochrome p450 isoenzymes is a major cause of drug interaction. Some examples are given in Box 1.1. Thus, for example, warfarin is metabolized by CYP2C9. Between 2 and 10% of people are homozygous for an allele that results in low enzyme activity and this leads to higher plasma warfarin levels.
The variability of a drug’s action within the body is partly due to the drug receptor and the polymorphism of this receptor.
Prescribing for the elderly
Table 1.2 Common adverse effects of drugs in the elderly
| Drug | Effect |
|---|---|
| β-Blockers (including eye drops) Digoxin | Bradycardia |
| Nitrates α-Adrenoceptor-blockers Diuretics | Postural hypotension |
| Diuretics (thiazides) | Glucose intolerance, gout |
| Antimuscarinic drugs Tricyclic antidepressants Neuroleptics Minor tranquillizers Anticonvulsants Hypnotics Opioids | Confusion, cognitive dysfunction |
| Bisphosphonates (mainly alendronic acid) | Oesophageal ulceration and stricture formation |
| NSAIDs | Gastric erosions Upper gastrointestinal bleeding Perforated peptic ulcer Renal impairment |
Prescribing in pregnancy/breast feeding
Never prescribe a drug to pregnant women unless it is absolutely necessary and you have checked for possible teratogenic effects on the fetus. Appendix A gives websites for drug use. If a known teratogenic drug is required during pregnancy (e.g. an anticonvulsant), always discuss the adverse effects on the fetus with the parents, preferably prior to conception.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


