CHAPTER 31 Infratemporal and pterygopalatine fossae and temporomandibular joint
INFRATEMPORAL FOSSA
The infratemporal fossa has a roof, and lateral and medial walls, and is open to the neck posteroinferiorly, i.e. the fossa has no anatomical floor. The roof is formed by the infratemporal surfaces of the temporal bone and of the greater wing of the sphenoid, and contains the foramena ovale and spinosum and the petrotympanic fissure: it is open superiorly to the temporal fossa. The medial wall is formed anteriorly by the lateral pterygoid plate of the pterygoid process of the sphenoid, and more postero-medially by the pharynx and tensor and levator veli palatini. It contains the pterygomaxillary fissure across which structures pass between the infratemporal and pterygopalatine fossae (Fig. 31.1). The lateral wall is formed by the medial surface of the ramus of the mandible.
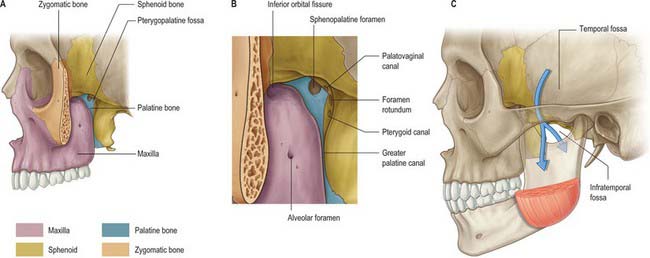
Lateral pterygoid provides a key to understanding the relationships of structures within the infratemporal fossa. This muscle lies in the roof of the fossa and runs anteroposteriorly in a more or less horizontal plane from the region of the pterygoid plates to the mandibular condyle (Fig. 31.1). Branches of the mandibular nerve and the main origin of medial pterygoid are deep relations and the maxillary artery is superficial. The buccal branch of the mandibular nerve passes between the two heads of lateral pterygoid. Medial pterygoid and the lingual and inferior alveolar nerves emerge below its inferior border and the deep temporal nerves and vessels emerge from its upper border. A venous network, the pterygoid venous plexus, lies around and within lateral pterygoid and is important in the spread of infection.
BONES
The sphenoid bone, the paired maxillae and temporal bones, and the mandible, collectively provide the skeletal framework to the infratemporal and pterygopalatine regions. The mandible and the two temporal bones articulate at the right and left temporomandibular joints. The disarticulated maxilla is described in Chapter 29, the temporal bone is described in Chapter 36, and the sphenoid and mandible are described here.
Sphenoid bone
The sphenoid bone lies in the base of the skull between the frontal, temporal and occipital bones. It has a central body, paired greater and lesser wings that spread laterally from the body, and two pterygoid processes that descend from the junction of the body and greater wings (Fig. 31.2).

Fig. 31.2 Sphenoid bone. A, anterior view; B, posterior view; C, superior view.
(From Sobotta 2006.)
Body
The body of the sphenoid is cuboidal. It contains two air sinuses, separated by a septum (see Ch. 32). Its cerebral (superior) surface articulates in front with the cribriform plate of the ethmoid bone. Anteriorly is the smooth jugum sphenoidale, which is related to the gyri recti and olfactory tracts. The jugum is bounded behind by the anterior border of the sulcus chiasmatis, which leads laterally to the optic canals. Posteriorly is the tuberculum sellae, behind which is the deeply concave sella turcica. In life the sella contains the hypophysis cerebri in the hypophysial fossa. Its anterior edge is completed laterally by two middle clinoid processes, while posteriorly the sella turcica is bounded by a square dorsum sellae, the superior angles of which bear variable posterior clinoid processes. The diaphragma sella and the tentorium cerebelli are attached to the clinoid processes (see Ch. 27). On each side, below the dorsum sellae, a small petrosal process articulates with the apex of the petrous part of the temporal bone. The body of the sphenoid slopes directly into the basilar part of the occipital bone posterior to the dorsum sellae, together these bones form the clivus. In the growing child this is the site of the spheno-occipital synchondrosis: premature closure of this joint gives rise to the skull appearances seen in achondroplasia.
The lateral surfaces of the body are united with the greater wings and the medial pterygoid plates. A broad carotid sulcus accommodates both the internal carotid artery and the cranial nerves associated with the cavernous sinus above the root of each wing (see Ch. 27). The sulcus is deepest posteriorly. It is overhung medially by the petrosal part of the temporal bone and has a sharp lateral margin, the lingula, which continues back over the posterior opening of the pterygoid canal.
A median triangular, bilaminar sphenoidal crest on the anterior surface of the body of the sphenoid makes a small contribution to the nasal septum. The anterior border of the crest joins the perpendicular plate of the ethmoid bone, and a sphenoidal sinus opens on each side of it (see Ch. 32). In the articulated state the sphenoidal sinuses are closed anteroinferiorly by the sphenoidal conchae, which are largely destroyed when disarticulating a skull. Each half of the anterior surface of the body of the sphenoid possesses a superolateral depressed area joined to the ethmoid labyrinth which completes the posterior ethmoidal sinuses; a lateral margin which articulates with the orbital plate of the ethmoid above and the orbital process of the palatine bone below; and an inferomedial, smooth, triangular area, which forms the posterior nasal roof, and near whose superior angle lies the orifice of a sphenoidal sinus.
Superior orbital fissure
The superior orbital fissure connects the cranial cavity with the orbit. It is bounded medially by the body of the sphenoid, above by the lesser wing of the sphenoid, below by the medial margin of the orbital surface of the greater wing, and laterally, between the greater and lesser wings, by the frontal bone. The contents of the superior orbital fissure are described in Chapter 39.
Sphenoidal conchae
Anterior parts of the two bones meet in the midline, and protrude as the sphenoidal crest. The horizontal part appears in the nasal roof and completes the sphenopalatine foramen. Its medial edge articulates with the rostrum of the sphenoid and the ala of the vomer. Its apex, directed posteriorly, is superomedial to the vaginal process of the medial pterygoid plate and joins the posterior part of the ala. A small conchal part sometimes appears in the medial wall of the orbit, lying between the orbital plate of the ethmoid in front, the orbital process of the palatine bone below and the frontal bone above.
Mandible
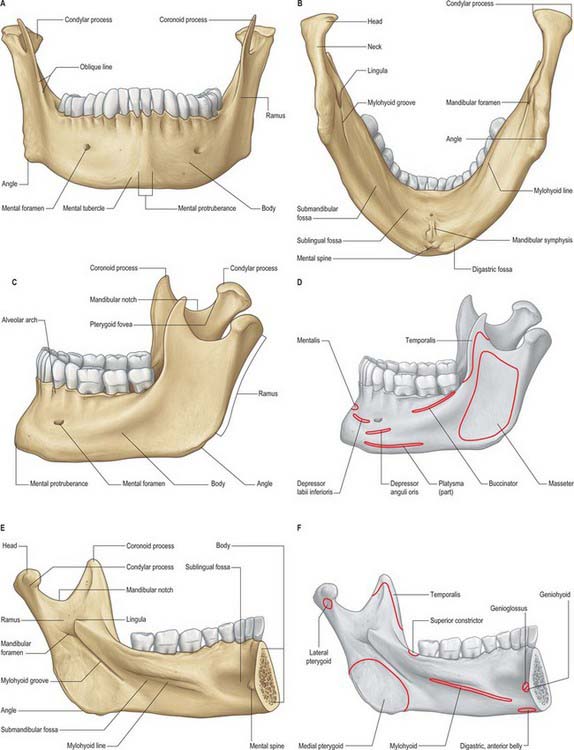
The mandible is the largest, strongest and lowest bone in the face. It has a horizontally curved body that is convex forwards, and two broad rami that ascend posteriorly (Fig. 31.3). The body of the mandible supports the mandibular teeth within the alveolar process. The rami bear the coronoid and condylar processes. Each condyle articulates with the adjacent temporal bone at the temporomandibular joint.
Body
The upper border, the alveolar part, contains 16 alveoli for the roots of the lower teeth. It consists of buccal and lingual plates of bone joined by interdental and inter-radicular septa. Near the second and third molar teeth the external oblique line is superimposed upon the buccal plate. Like the maxilla, the form and depth of the tooth sockets is related to the morphology of the roots of the mandibular teeth. The sockets of the incisor, canine and premolar teeth usually contain a single root, while those for the three molar teeth each contain two or three roots. The third molar is variable in its position and root presentation. It may be impacted vertically, horizontally, mesially or distally, and its roots may be bulbous, hooked, divergent or convergent, and occasionally embrace the mandibular (inferior dental) canal (see Ch. 30). The internal surface of the mandible is divided by an oblique mylohyoid line that gives attachment to mylohyoid (and, above its posterior end, to the superior pharyngeal constrictor, some retromolar fascicles of buccinator, and the pterygomandibular raphe behind the third molar). The mylohyoid line extends from a point approximately 1 cm from the upper border behind the third molar as far forwards as the mental symphysis; it is sharp and distinct near the molars, but faint further forwards. The mylohyoid groove extends downwards and forwards from the ramus below the posterior part of the mylohyoid line and contains the mylohyoid neurovascular bundle. The area below the line is a slightly concave submandibular fossa and is related to the submandibular gland. The area above the line widens anteriorly into a triangular sublingual fossa and is related to the sublingual gland: the bone is covered by oral mucosa above the sublingual fossa as far back as the third molar. In an edentulous subject it may be necessary to reduce any ridge-like prominence of the mylohyoid line in order that dentures may fit without traumatizing the overlying oral mucosa.
Ramus
The mandibular ramus is quadrilateral, and has two surfaces (lateral and medial), four borders (superior, inferior, anterior and posterior) and two processes (coronoid and condylar). The lateral surface is relatively featureless and bears the (external) oblique ridge in its lower part. The medial surface presents, a little above centre, the mandibular foramen, through which the inferior alveolar neurovascular bundle passes to gain access to the mandibular canal (see below). Anteromedially, the mandibular foramen is overlapped by a thin, sharp triangular spine, the lingula, to which the sphenomandibular ligament is attached, and which is also the landmark for an inferior alveolar local anaesthetic block injection. Below and behind the foramen, the mylohyoid groove runs obliquely downward and forward.
Ossification
The mandible forms in dense fibromembranous tissue lateral to the inferior alveolar nerve and its incisive branch, and also in the lower parts of Meckel’s cartilage (first branchial arch). Each half is ossified from a centre that appears near the mental foramen about the sixth week in utero. From this site, ossification spreads medially and posterocranially to form the body and ramus, first below, and then around, the inferior alveolar nerve and its incisive branch. Ossification then spreads upwards, initially forming a trough, and later crypts, for the developing teeth. By the tenth week, Meckel’s cartilage below the incisor rudiments is surrounded and invaded by bone. Secondary cartilages appear later (Fig. 31.4): a conical mass, the condylar cartilage, extends from the mandibular head downwards and forwards in the ramus, and contributes to its growth in height. Although it is largely replaced by bone by midfetal life, its proximal end persists as proliferating cartilage under the fibrous articular lining until about the third decade. Another secondary cartilage, which soon ossifies, appears along the anterior coronoid border, and disappears before birth. One or two cartilaginous nodules also occur at the symphysis menti. At about the seventh month in utero these may ossify as variable mental ossicles in symphysial fibrous tissue: they unite with adjacent bone before the end of the first postnatal year.

Age changes in the mandible
At birth the two halves of the mandible are united by a fibrous symphysis menti (Fig. 31.5). The anterior ends of both rudiments are covered by cartilage, separated only by a symphysis. Until fusion occurs, new cells are added to each cartilage from symphysial fibrous tissue, and ossification on its mandibular side proceeds towards the midline. When the latter process overtakes the former, and ossification extends into median fibrous tissue, the symphysis fuses. At this stage the body is a mere shell which encloses the imperfectly separated sockets of deciduous teeth. The mandibular canal is near the lower border, and the mental foramen opens below the first deciduous molar and is directed forwards. The coronoid process projects above the condyle.
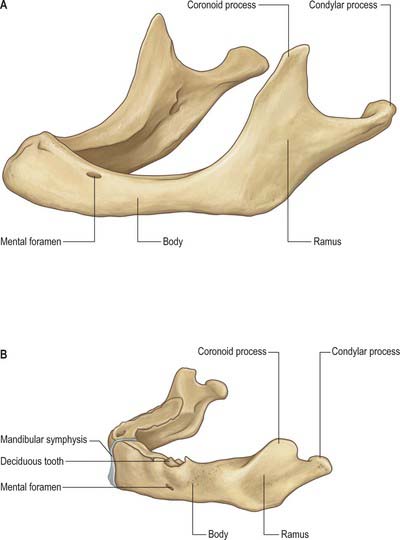
Fig. 31.5 A, Edentulous mandible; note position of mental foramen; B, Neonatal mandible.
(Redrawn with permission from Sobotta 2006.)
In general terms, increase in height of the body of the mandible is achieved primarily by formation of alveolar bone associated with the developing and erupting teeth, although some bone is also deposited on the lower border. Increase in length of the mandible is accomplished by deposition of bone on the posterior surface of the ramus and concomitant compensatory resorption on the anterior surface (accompanied by deposition of bone on the posterior surface of the coronoid process and resorption on the anterior surface of the condylar process). Increase in width of the mandible is produced by deposition of bone on the outer surface of the mandible and resorption on the inner surface. An increase in the comparative size of the ramus compared with the body of the mandible occurs during postnatal growth and tooth eruption.
In adults, alveolar and subalveolar regions are about equal in depth, and the mental foramen appears midway between the upper and lower borders. If teeth are lost, alveolar bone is resorbed, which means that the mandibular canal (which runs parallel to the mylohyoid line) and the mental foramen come to lie much nearer to the superior border (Fig. 31.5), indeed, sometimes they may both disappear, so that the nerves lie just beneath the oral mucosa.
TEMPOROMANDIBULAR JOINT
It is probably impossible to measure the pressure developed on the articular surfaces of the human jaw joint when biting, however direct measurement of loads across the joint in animals has demonstrated significant intermittent loading during mastication. There is also irrefutable theoretical evidence based on Newtonian mechanics that the jaw joint is a weight-bearing joint. With a vertical bite force of 500 N on the left first molar, the right condyle must support a load of well over 300 N (Osborn 1995a). The non-working condyle is more loaded than the condyle on the working side, which may help explain why patients with a fractured condyle choose to bite on the side of the fracture.
Fibrous capsule
The lower part of the joint is surrounded by tight fibres which attach the condyle of the mandible to the disc. The upper part of the joint is surrounded by loose fibres which attach the disc to the temporal bone (Fig. 31.6
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


