IgA Acute Glomerulonephritis Associated with S. Aureus
Robert B. Colvin, MD
Key Facts
Etiology/Pathogenesis
Staphylococcus aureus, coagulase positive, often MRSA
Increased risk with diabetes mellitus, neoplasia, old age
Clinical Issues
Infection, septicemia
Acute renal failure
Proteinuria, nephrotic range (20-80%)
Purpura
˜ 25% of biopsies with acute postinfectious glomerulonephritis
Microscopic Pathology
Glomerular involvement varies from mild mesangial hypercellularity to marked acute inflammation with crescents
Red cell casts common
Focal interstitial nephritis
Ancillary Tests
IgA dominant or codominant immunoglobulin, mostly mesangial
EM deposits primarily mesangial and paramesangial
Occasional subepithelial “humps”
“Humps” sometimes have “cups” in contrast to poststreptococcal GN
Occasional subendothelial deposits
Top Differential Diagnoses
IgA nephropathy
Henoch-Schönlein purpura
Acute glomurelonephritis from other causes
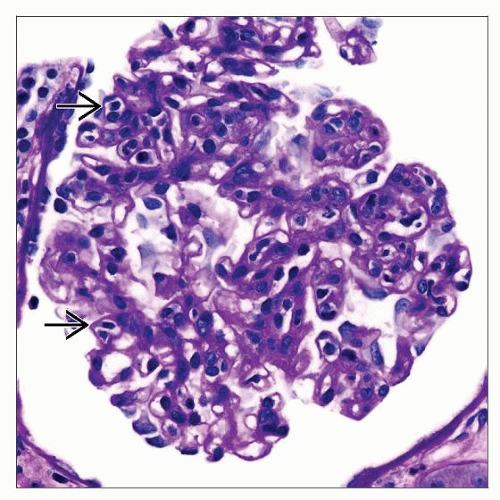 Glomerulitis may be mild in cases of IgA positive acute glomerulitis associated with Staphylococcus aureus infection. Many mononuclear and a few polymorphonuclear leukocytes are present  . . |
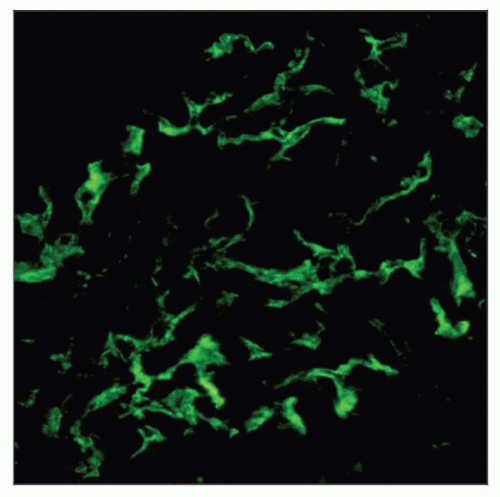 Acute glomerulonephritis associated with Staphylococcal aureus infection typically has prominent mesangial IgA deposits, which resemble IgA nephropathy or HSP. |
TERMINOLOGY
Definitions
Acute glomerulonephritis (GN) associated with Staphylococcus aureus infection with predominance of IgA deposition
ETIOLOGY/PATHOGENESIS
Infectious Agents
S. aureus, coagulase positive, often methicillin resistant (MRSA)
Osteomyelitis, pneumonia, septic arthritis, discitis, soft tissue abscess, empyema, sinusitis, endocarditis
Septicemia
Not usually postinfectious GN but occurs during chronic infection
Average duration of infection is 5 weeks
Host Factors
Diabetes mellitus, neoplasia, old age, alcoholism
Immune Response
IgA antibodies to S. aureus cell membrane antigen (GenBank BAB41819.1)
S. aureus enterotoxins may act as superantigens, stimulating T cells and leading to polyclonal B-cell activation
1 superantigen-like protein (SSL7) binds to Fc of IgA, blocking FcR activity
CLINICAL ISSUES
Presentation
Persistent infection, septicemia
Acute renal failure
Hematuria
Proteinuria, nephrotic range (20-80%)
Hypertension
Hypocomplementemia (minority)
Purpura
Treatment
Antibiotics and renal support
Anecdotal reports of steroids/immunosuppression
Prognosis
Data limited
Range of outcomes from complete recovery to ESRD
Recovery possible if infection successfully treated
Underlying disease and age are important factors
Prevalence
˜ 25% of renal biopsies with acute postinfectious glomerulonephritis
MICROSCOPIC PATHOLOGY
Histologic Features
Glomerulus
Varies from mild mesangial hypercellularity to marked acute inflammation with crescents
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


