19 Hypertension
The cardiovascular complications associated with hypertension are shown in Box 19.1. The most common and important of these are stroke and myocardial infarction. An increase of 5 mmHg in usual diastolic blood pressure is associated with a 35–40% increased risk of stroke. There is a similar but less steep association for coronary heart disease risk. The risk of heart failure is increased six-fold in hypertensive subjects. Meta-analysis of clinical trials has indicated that these risks are reversible with relatively modest reductions in blood pressure of 10/6 mmHg associated with a 38% reduction in stroke and 16% reduction in coronary events (Collins et al., 1990), while a 5 mmHg reduction in blood pressure is associated with a 25% reduction in risk of renal failure.
The absolute benefits of blood pressure lowering achieved as a result of these relative risk reductions depend on the underlying level of risk in an individual. High-risk subjects gain more benefit in terms of events saved per year of therapy. Absolute risk is highest in those who already have evidence of cardiovascular disease, such as previous myocardial infarction, transient ischaemic attack or stroke, or who have other evidence of cardiovascular dysfunction such as electrocardiogram (ECG) or echocardiograph abnormality. Risk is also increased in the elderly and in people with diabetes or renal failure and is further enhanced by other risk factors such as smoking, dyslipidaemia, obesity and sedentary lifestyle. In those under the age of 75, men are at greater risk than women. Cardiovascular risk in an individual who has no current cardiovascular disease can be estimated from coronary risk prediction charts (Joint British Societies, 2005; see Chapter 24).
Epidemiology
In 90–95% of cases of hypertension, there is no underlying medical illness to cause high blood pressure. This is termed ‘essential’ hypertension, so named because at one time it was erroneously believed to be an ‘essential’ compensation mechanism to maintain adequate circulation. The precise aetiology of essential hypertension is currently unknown. Genetic factors clearly play a part as the condition clusters in families, with hypertension being twice as common in subjects who have a hypertensive parent. Genetic factors account for about one-third of the blood pressure variation between individuals, although no single gene appears to be responsible except in some rare conditions such as polycystic kidney disease and other metabolic conditions such as Liddle’s syndrome (Beevers et al., 2001). The remaining 5–10% of cases are secondary to some other disease process (Box 19.2).
Box 19.2 Causes of hypertension
Secondary hypertension (5–10%)
Management of hypertension
In the UK, the management of hypertension is guided by consensus guidelines produced by the British Hypertension Society (BHS) and the National Institute for Health and Clinical Excellence (NICE). In 2004, there were significant differences between NICE and BHS guidance but these were addressed in the form of modified joint guidance issued in 2006 which specifically addressed the areas of controversy (National Collaborating Centre for Chronic Conditions: Hypertension, 2006). The European Society of Hypertension also published a task force discussion document in January 2009 and formal guidance in 2007 (Mancia et al., 2009).
Assessment of the hypertensive patient
Contributing factors
The patient should also be assessed for possible contributory factors to hypertension such as obesity, excess alcohol or salt intake and lack of exercise. Occasionally, hypertension may be provoked by the use of drugs (see Box 19.2), including over-the-counter medicines used as cold and flu remedies. Other risk factors should also be documented and addressed, for example, smoking, diabetes and hyperlipidaemia. It is important to establish whether there is a family history of cardiovascular disease.
Determination of cardiovascular risk
An accurate assessment of cardiovascular disease risk is essential before recommending appropriate management in hypertension. Patients with documented atheromatous vascular disease, for example, previous myocardial infarction or stroke, angina or peripheral vascular disease are at high risk of recurrent events. Those with type 2 diabetes over 40 years of age are also at high risk and can be regarded as ‘coronary equivalents’, that is, with risks similar to non-diabetic patients with previous myocardial infarction. For non-diabetic patients without vascular disease it is necessary to estimate cardiovascular risk (see Chapter 24). A 10-year cardiovascular disease risk of 20% (equivalent to a 15% coronary heart disease risk) is regarded as an appropriate threshold for antihypertensive therapy in patients with moderate hypertension, as well as for lipid-lowering therapy. Treatment decisions based on these tables will favour treatment in elderly subjects. While a younger patient may be at lower absolute risk over 10 years and may not meet the criteria for blood pressure and lipid treatment, they may be at higher lifetime and longer term risk of premature death and vascular disease and, thus, still merit risk factor intervention.
Other factors to consider include microalbuminuria which increases cardiovascular risk by a factor of 2–3 and the combination of reduced GFR and microalbuminuria may increase risk by as much as six-fold (Cirillo et al 2008; Sehestedt et al., 2009).
Treatment
Non-pharmacological approaches
Non-pharmacological management of hypertension is important, although the effects are often disappointing. Patients with mild hypertension in the range 140–159/90–100 mmHg can be assessed for levels of risk while offered lifestyle advice. General health education is important to allow patients to make informed choices about management. In order to maximise potential benefit, patients should receive clear and unambiguous advice, including written information they can digest in their own time. Written advice for patients can be downloaded from the BHS website (http://www.bhsoc.org/).
In patients who are overweight, weight loss results in reduction in blood pressure of about 2.5/1.5 mmHg/kg. The DASH diet (Dietary Approaches to Stop Hypertension) was evaluated in a clinical trial and found to lower blood pressure significantly (4.5/2.7 mmHg) compared with a typical US diet. This diet emphasises fruit, vegetables, and low-fat dairy produce in addition to fish, low-fat poultry and whole grains while minimising red meat, confectionary and sweetened drinks (Appel et al., 1997). Subjects should reduce their salt intake, for example, by not adding salt to food on the plate. A daily sodium intake of <100 mmol (i.e. 6 g sodium chloride or 2.4 g elemental sodium) should be the aim. There is a significant amount of hidden salt in processed meat, ready meals, cheese and even bread. A dietary assessment may be required to accurately quantify a patient’s salt intake and advise on how reductions might be made.
Drug treatment
Treatment thresholds
Treatment thresholds are summarised in Table 19.1. Lifestyle advice should be provided to all patients with any degree of hypertension. Patients with severe hypertension (>220/120 mmHg confirmed on several readings on the same occasion) should be treated immediately and some guidance suggests that dual therapy should be commenced immediately in patients with blood pressure >20 mmHg above their target as monotherapy is unlikely to be fully effective (Mancia et al., 2007). Patients with blood pressures in the range 160–220/100–120 mmHg should be monitored over several weeks and treated if blood pressure remains in this range. The period of observation before starting treatment depends on the severity of the hypertension and the presence or absence of end-organ damage (see Table 19.1). Patients whose blood pressure is in the range 140–159/90–99 mmHg should be observed annually unless they have evidence of target organ damage, cardiovascular complications, diabetes or a calculated cardiovascular risk >20% over 10 years, in which case drug treatment should be offered. Patients with blood pressure in the range 135–139/85–89 mmHg should be reassessed annually, while those with blood pressure lower than this can be rechecked every 5 years.
Table 19.1 Threshold blood pressures for intervention
| Initial blood pressure | Management | |
|---|---|---|
| Systolic (mmHg) | Diastolic (mmHg) | |
| Malignant hypertension | Admit and treat immediately | |
| >220 | >120 | Repeat several times at the same attendance and treat immediately if blood pressure persists in this range |
| 180–219 | 110–119 | Confirm over 1–2 weeks and treat if blood pressure remains in this range |
| 160–179 | 100–109 | Repeat over 3–4 weeks (end-organ damage present) or 2–12 weeks (no end-organ damage), institute non-pharmacological measures and treat if blood pressure persists in this range |
| 140–159 | 90–99 | Repeat over several weeks. Institute non-pharmacological measures. Treat if remains in this range and patient has target organ damage, cardiovascular complications or an estimated 10-year cardiovascular risk >20%. Otherwise reassess annually |
| 135–139 | 85–89 | Reassess annually |
| <135 | <85 | Reassess in 5 years |
Target blood pressures
Within the Hypertension Optimal Treatment (HOT) study (Hansson et al., 1998), patients were allocated diastolic target blood pressures of <90, 85, 80 mmHg. The study struggled to stratify patients effectively into these treatment groups but analysis suggested that the optimum target blood pressure was <140/85 mmHg with little benefit in lowering to lower levels of 120/70 mmHg but also little evidence of harm.
The UK Prospective Diabetes Study Group (1998a,b) suggested ‘tight’ blood pressure control was better than less tight in patients with non-insulin-dependent diabetes. The targets in the UK Prospective Diabetes Study were ‘tight’ <150/85 mmHg and ‘less tight’ <180/105 mmHg but the actually achieved blood pressures were lower, for example, 154/87 mmHg versus 144/82 mmHg. Recommendations in diabetics have, therefore, suggested treating to a target of 140/80 mmHg or less, although few studies have successfully lowered blood pressure to these levels.
A more recent study (Cardio-Sis) randomised non-diabetic subjects with systolic blood pressure >150 mmHg to target systolic blood pressure of <140 or <130 mmHg (Verdecchia et al., 2009). The primary end-point was left ventricular hypertrophy though the secondary end-point of a composite cardiovascular end-point was reduced (as well as the primary end-point) in the 130-mmHg group, with no increase in adverse events. This, however, is not robust enough evidence to recommend a reduction in blood pressure target levels and would require a larger study of hard clinical end-points to confirm these findings.
Achievement of target blood pressures is incorporated as a quality indicator for the General Medical Services Contract for primary care doctors in the UK. Diabetic patients are an exception and benefit from more aggressive blood pressure reduction. Target blood pressures for diabetic and non-diabetic subjects are summarised in Table 19.2. It should be emphasised that the audit standard will not be achieved in all patients.
Table 19.2 Target clinic blood pressures according to British Hypertension Society guidelines 2004 (Williams et al., 2004)
| Clinic blood pressure | ||
| No diabetes (mmHg) | Diabetes (mmHg) | |
| Optimal treated blood pressure | <140/85 | <130/80 |
| Audit standard | <150/90 | <140/80 |
Antihypertensive drug classes
β-Adrenoreceptor antagonists
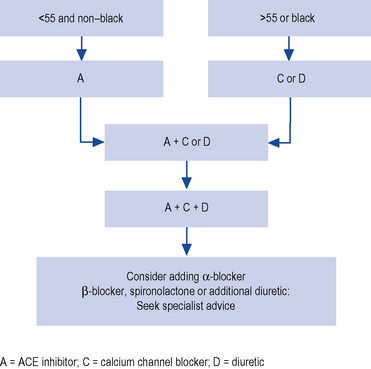
β-Adrenoreceptor antagonists also have substantial clinical trial evidence of benefit over placebo in hypertension, and are relatively inexpensive. However, their use is declining and they have been relegated to fourth-line therapy in the UK according to NICE guidance (Fig. 19.1). This recommendation largely stems from the evidence that they may be less effective at preventing stroke in conjunction with their diabetogenic effects. The Losartan For Endpoint reduction in hypertension (LIFE) study compared an atenolol/thiazide-based regime with a losartan-based regime and demonstrated equivalent levels of blood pressure reduction but with a small excess incidence of stroke in the atenolol arm (Dahlöf et al., 2002). In the Anglo Scandinavian Cardiac Outcomes Trial (ASCOT) study, the risk of diabetes was 2.5% higher in the atenolol arm compared with the amlodipine arm with similar increased risk of diabetes found within the atenolol arm of the LIFE study (Dahlöf et al., 2005). A Cochrane review warned of the excess risk in developing diabetes in patients prescribed combinations of thiazide diuretics and β-blockers. This would equate to one new case per 500 treated (Mason et al., 2004). The combination of thiazide and a β-blocker should, therefore, be avoided if possible, particularly in those who are at risk of developing diabetes (e.g. obese, strong family history of diabetes, South Asian origin).
To complicate matters, however, a long-term 20-year follow-up study of the UKPDS study found similar cardiovascular outcomes between patients on β-blockers and ACE inhibitors with a reduction in all causes of mortality which actually favoured β-blockers (Holman et al., 2008). β-Blockers do remain most suitable for younger hypertensives who have another indication for β-blockade, such as coronary heart disease. β-Blockers are also effective in suppressing atrial fibrillation and this may be one group of patients where first-line therapy with β-blockers is still merited.



