Hodgkin Lymphoma
Key Facts
Clinical Issues
HL arising primarily in lungs is extremely rare
Pulmonary involvement is most often seen in course of regional or systemic dissemination
Night sweats
Mediastinal, cervical, or supraclavicular lymphadenopathy
Microscopic Pathology
Majority of cases are of nodular sclerosis subtype and rest are of mixed cellularity
Nodules consist of varying numbers of lymphocytes, plasma cells, and eosinophils admixed with scattered Reed-Sternberg cells
Neoplastic cells are represented by transformed atypical lymphocytes (Hodgkin cells and Reed-Sternberg cells)
Hodgkin cells (HC) are large, mononuclear cells with large nucleus containing single prominent eosinophilic nucleolus
Reed-Sternberg cells (RSC) are bi- or multinucleated cells containing prominent eosinophilic nucleoli
Neoplastic cells always represent minority of infiltrate (0.1-10% of cells in infiltrate)
Ancillary Tests
Reed-Sternberg cells and their variants show strong membranous and paranuclear (Golgi zone) positivity for CD30 and CD15
Reed-Sternberg cells shows weak positivity for Pax-5 and can express EBV-encoded LMP-1
Reed-Sternberg cells are negative for CD45, CD79a, and, in a majority of cases, CD20
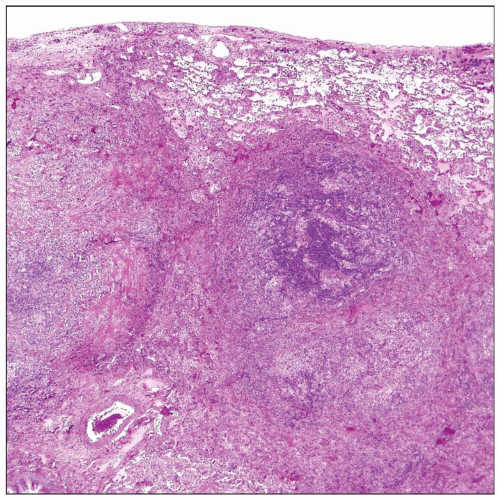 Multiple tumor nodules are seen in this lung involved with Hodgkin lymphoma. The infiltrate is composed of a mixed population of lymphocytes, plasma cells, eosinophils, and scattered large atypical cells. |
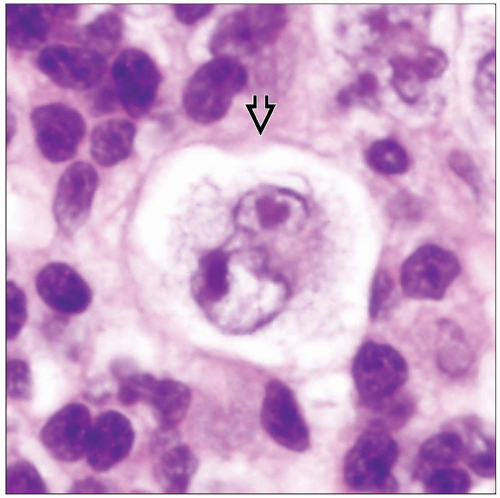 High magnification of a pulmonary nodule in Hodgkin lymphoma shows a characteristic binucleated Reed-Sternberg cell with double nuclei and prominent “owl-eyed” eosinophilic nucleoli  . . |
TERMINOLOGY
Abbreviations
Hodgkin lymphoma (HL)
Synonyms
Hodgkin disease
Definitions
Lymphoid neoplasm composed of scattered mononuclear and multinucleated atypical lymphoid cells amid a mixed lymphoreticular infiltrate
ETIOLOGY/PATHOGENESIS
Pathogenesis
Epstein-Barr virus (EBV) has been claimed to play a role in subset of cases
EBV infection may be cofactor in the genetic cascade of events leading to development of HL
Neoplastic cells are derived from mature B cells at the germinal center stage of differentiation in > 98% of cases
CLINICAL ISSUES
Epidemiology
Incidence
HL arising primarily in lungs is extremely rare
Pulmonary involvement is most often seen in course of regional or systemic dissemination
Age
Bimodal age distribution with peak incidences between 20-30 years and 60-80 years
Presentation
Night sweats
Mediastinal, cervical, or supraclavicular lymphadenopathy
Treatment
Adjuvant therapy
Combination chemotherapy
Prognosis
Primary extranodal pulmonary HL tends to follow more aggressive behavior than nodal-based HL
IMAGE FINDINGS
General Features
Morphology
Single or multiple nodules
Bilateral reticulonodular infiltrates are seen less frequently
Absence of associated lymphadenopathy in primary lung cases
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


