Figure 8-1 Heart failure (HF) classification by disease stage with appropriate therapeutic goals. ACEI, angiotensin-converting enzyme inhibitor; ARB, angiotensin receptor blocker; AF, atrial fibrillation; CAD, coronary artery disease; CRT, Cardiac resynchronization therapy; DM, diabetes mellitus; EF, ejection fraction; HTN, hypertension; ICD, implantable cardioverter-defibrillator; LV, left ventricular; LVH, left ventricular hypertrophy; MI, myocardial infarction; GDMT, guideline-directed medical therapy; HRQOL, health-related quality of life; MCS, mechanical circulatory support. Modified from: Yancy CW, Jessup M, Bozkurt B, et al. 2013 ACCF/AHA guideline for the management of heart failure: a report of the American College of Cardiology Foundation/American Heart Association Task Force on practice guidelines. Circulation 2013;128:e240–e327.
Epidemiology
- HF afflicts more than 6 million people in the United States. At 40 years of age, the lifetime risk of developing HF for both men and women is one in five. HF incidence approaches 10 per 1,000 population after 65 years of age. Greater than 10% of deaths in the United States have HF mentioned on the death certificate.2
- Up to 30% of patients hospitalized with an HF exacerbation will be rehospitalized within the subsequent 3 months.3
- Mortality from HF ranges from 10% to 50% within 1 year of diagnosis depending on disease severity.1,3
- Up to 50% of patients who present with clinical HF have preserved left ventricular (LV) systolic function (EF ≥40%); this entity is known as heart failure with preserved ejection fraction (HFPEF). Three-month mortality is similar in patients with preserved or reduced LV systolic function.4 The mortality rate for HFPEF at 3 months following index hospitalization is approximately 10%, and the 5-year mortality is >50%.
Etiology
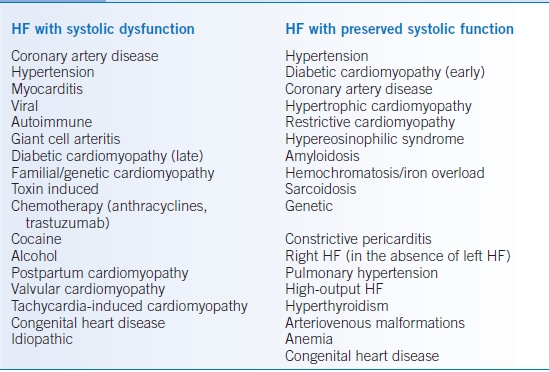
- The potential causes of HF are diverse. In the United States, coronary artery disease (CAD), hypertension (HTN), and diabetes mellitus (DM) are the most common disorders leading to cardiac dysfunction. CAD is less common in the HFPEF population when compared to those with systolic dysfunction.
- The differential diagnosis for HF according to LV systolic function is shown in Table 8-1.
TABLE 8-1 Causes of Heart Failure
Risk Factors
- Recognition of patients at risk for HF is important. The early initiation of behavioral interventions and HF therapies can significantly improve patient outcomes and delay or prevent the onset of clinical disease.
- The primary modifiable risk factors associated with HF are HTN, DM, and CAD; therefore, identification and treatment of these diseases and their risk factors (e.g., smoking, obesity, physical inactivity, dyslipidemia) are critical.
- Other factors associated with increased risk of HF include a family history of cardiomyopathy and exposure to cardiotoxins such as chemotherapy drugs (especially anthracyclines and trastuzumab), alcohol, or illicit drugs (especially cocaine).
- HFPEF is more common in women, in elderly patients, and in those with HTN, and common comorbidities include atrial fibrillation, renal insufficiency, and DM.4
Pathophysiology
- HF is the consequence of an acute or chronic injury or stress imposed on one or more cardiac structures that leads to impaired cardiac function and diminished cardiac reserve.
- During the course of HF, the renin-angiotensin-aldosterone system (RAAS), the sympathetic nervous system, and the vasopressin system are activated to maintain normal cardiac output and tissue perfusion. However, these initially adaptive neurohumoral pathways ultimately lead to further cardiac injury, fibrosis, and LV dilation. This process is known as adverse myocardial remodeling.
DIAGNOSIS
HF is a clinical diagnosis based on patient symptoms and physical findings consistent with cardiac dysfunction. Laboratory testing and echocardiography are also important tools to aid in the diagnosis and characterization of patients presenting with HF syndromes. HFPEF and HF with reduced ejection fraction (HFREF) cannot be reliably distinguished by history and physical examination alone.
Clinical Presentation
History
- Shortness of breath, including breathlessness during activity, at rest, or while sleeping (paroxysmal nocturnal dyspnea; PND). Patients often have difficulty breathing while lying flat and may need to elevate their upper body on pillows (orthopnea).
- Swelling in the feet, ankles, legs, or abdomen, which can be associated with weight gain. Patients may find that their shoes feel tight.
- Abdominal swelling, and decreased blood flow to the digestive system, can be associated with decreased appetite, nausea, or early satiety.
- Persistent coughing or wheezing, particularly coughing that produces white or pink-tinged mucous from fluid backup in the lungs.
- Generalized fatigue and memory loss and disorientation can also occur.
- The history should evaluate for potential causes:
- Ischemic heart disease: chest pain, history of myocardial infarction (MI), presence of CAD risk factors
- Myocarditis: recent viral illness, rheumatologic symptoms
- Genetic cardiomyopathy: family history of HF or sudden death
- Toxic cardiomyopathy: history of chemotherapy, alcohol or drug abuse
- Hypertensive cardiomyopathy: history of HTN and inadequate blood pressure control
- Diabetic cardiomyopathy: personal or family history of DM, obesity, polyuria
- Peripartum cardiomyopathy: recent pregnancy
- Constrictive pericarditis: history of chest irradiation or pericarditis
- Valvular heart disease: history of a heart murmur, rheumatic fever
- Infectious endocarditis: fever, chills, recent dental work, or other procedures
- Ischemic heart disease: chest pain, history of myocardial infarction (MI), presence of CAD risk factors
- Define the patient’s current functional status:
- How far can the patient walk before becoming short of breath?
- How many flights of stairs can the patient climb?
- Can the patient perform activities of daily living?
- Compare functional status with previous visits to assess for change.
- Determine the NYHA functional class.
- How far can the patient walk before becoming short of breath?
- Assess the patient’s volume status. Determine presence of PND, orthopnea, lower extremity (LE) edema, increased abdominal girth, and increased weight.
- Determine adherence to diet and medications:
- Inquire about intake of salt and high sodium foods.
- Ask about daily fluid intake.
- Inquire about medication use, side effects, and reasons for nonadherence (if applicable).
- Ask about use of any new medications (e.g., NSAIDs) or dietary supplements.
- Inquire about intake of salt and high sodium foods.
Physical Examination
- At each visit, heart rate, respiratory rate, blood pressure, and body weight should be reviewed to direct therapeutic changes.
- Another important function of the physical exam in an initial evaluation is to identify possible causes of HF (e.g., valvular disease, pericardial disease).
- Assessment of volume status on physical exam.
- Jugular venous distention (JVD): Defined as jugular venous pulse >3 to 4 cm above the sternal notch with the patient at 45 degrees. JVD usually correlates with elevated left-sided intracardiac filling pressures unless pulmonary HTN, pericardial constriction, or severe tricuspid regurgitation is present.
- S3: A low-frequency heart sound present following S2 that signifies impaired rapid, early diastolic filling of the LV. In patients with HF, this finding is specific but not sensitive for the presence of LV diastolic volume overload.
- Wet pulmonary crackles: A sign of fluid accumulation in the alveolar air spaces. Present only in about 50% of HF patients with elevated intracardiac filling pressures due to pulmonary lymphatic compensation. Crackles, usually dry, can also be present in other forms of lung disease (e.g., pneumonia, pulmonary fibrosis).
- Hepatomegaly/ascites: Reflects elevated central venous pressure (CVP) from right heart pressure or volume overload.
- LE pitting edema: A late sign of fluid overload that is approximately 30% sensitive for diagnosing hypervolemia in HF patients; not a specific sign of HF as many other diseases can produce LE edema.
- Narrow pulse pressure (<30 mm Hg) and pulsus alternans: Markers of significantly reduced cardiac stroke volume.
- Jugular venous distention (JVD): Defined as jugular venous pulse >3 to 4 cm above the sternal notch with the patient at 45 degrees. JVD usually correlates with elevated left-sided intracardiac filling pressures unless pulmonary HTN, pericardial constriction, or severe tricuspid regurgitation is present.
Diagnostic Testing
Laboratories
- Laboratory testing in HF can help in determining etiology but is more important for defining disease-modifying comorbidities such as DM, renal insufficiency, and anemia.
- The initial lab evaluation for all patients with newly diagnosed HF should include a complete blood cell count (CBC), basic metabolic panel (BMP), liver function tests, fasting lipid panel, fasting blood glucose, urinalysis (UA), and thyroid-stimulating hormone (TSH).
- In select patients with HF of unknown etiology, serum iron studies and tests for HIV and hepatitis C should also be considered.
- B-type natriuretic peptide (BNP) is released from myocytes in response to wall stress. A level >400 pg/mL is usually diagnostic of HF (in the absence of chronic kidney disease), whereas a level <100 pg/mL has a high negative predictive value for active HF. BNP levels have also been shown to correlate with the risk of future adverse events in HF patients. A BNP or N-terminal prohormone of brain natriuretic peptide (nt-proBNP) level is most useful when the diagnosis of HF is uncertain; levels may also be helpful for monitoring the clinical course and response to therapy and for assessing prognosis.
Electrocardiography
The 12-lead ECG is a useful point of care test to assess for evidence of myocardial ischemia or infarction, left ventricular hypertrophy (LVH), arrhythmias, and interventricular conduction delay (e.g., left bundle branch block [LBBB]).
Imaging
- The hallmarks of HF on chest radiography (CXR) are cardiomegaly, bilateral pulmonary infiltrates, and pleural effusions (R > L). In addition, the CXR evaluates for other potential causes of dyspnea such as pneumothorax, pneumonia, or chronic lung disease. Up to 50% of patients with chronic HF and elevated cardiac filling pressures have clear lung fields on CXR; therefore, this finding should not be used to exclude a diagnosis of HF.
- The echocardiogram is a critical component in the evaluation and management of HF.
- This imaging test provides information regarding LV and right ventricular (RV) systolic and diastolic function, LVH, valvular disease, pericardial disease, and pulmonary artery pressures.
- Diagnosis of HFPEF is usually based on echocardiographic criteria, mitral valve inflow, and tissue Doppler findings of normal LV systolic function with impaired diastolic function.
- Many aspects of HF disease management and prognosis are determined by the information obtained from the echocardiogram.
- This imaging test provides information regarding LV and right ventricular (RV) systolic and diastolic function, LVH, valvular disease, pericardial disease, and pulmonary artery pressures.
Diagnostic Procedures
- All patients with unexplained HF should have an evaluation for ischemia.
- Although not a standard test in the evaluation of HF, myocardial perfusion imaging (MPI) with thallium and sestamibi can be used in patients at lower risk for CAD to evaluate for ischemia. MPI may also be used to direct revascularization in patients with a known ischemic cardiomyopathy by identifying areas of ischemic but viable myocardium (i.e., hibernating myocardium).
- Similar to MPI, exercise or dobutamine infusion can be combined with echocardiography to assess exercise tolerance and/or identify active ischemia by detection of stress-induced wall motion abnormalities. A ramped dobutamine stress echo can also be used to assess myocardial viability in ischemic HF patients being evaluated for coronary bypass surgery.
- Coronary angiography is the gold standard for assessing occlusive coronary disease and should be considered unless the patient is a poor candidate (coagulopathy, renal failure, etc.) or the probability of CAD is very low.
- Newer imaging modalities may have a role in the initial assessment of HF. Both CT and magnetic resonance angiography could provide a noninvasive approach to evaluate for CAD in new-onset HF. Magnetic resonance imaging (MRI) also has potential value in identifying patients with myocarditis or other specific forms of cardiomyopathy (e.g., amyloidosis, sarcoidosis, arrhythmogenic right ventricular dysplasia [ARVD]). Additional studies are needed to define the role of these imaging techniques in HF.
- Routine endomyocardial biopsy for the evaluation of new-onset HF is not recommended. In most cases, the results are nondiagnostic and/or fail to impact management decisions. The use of endomyocardial biopsy can be considered in select patients in whom there is clinical suspicion for sarcoidosis, giant cell myocarditis, or amyloidosis.
TREATMENT
Chronic Heart Failure
- Numerous clinical trials have investigated pharmacologic therapy in chronic HF over the past 30 years. The results of these trials have led to the construction of detailed practice guidelines developed by the American College of Cardiology (ACC) and the American Heart Association (AHA) to help optimize outcomes in HF patients.1
- The goals of treatment are (1) to improve symptoms, maximize functional status, and improve quality of life; (2) to reduce mortality; (3) to minimize HF hospitalizations; and (4) to slow disease progression.
- Patients with ischemic or valvular cardiomyopathy should be evaluated for revascularization (via percutaneous intervention or surgery) and valve repair/replacement, respectively.
- The classification of HF patients into stages A to D can be used to direct the behavioral, pharmacologic, and device therapy that should be employed to reduce disease progression, hospitalizations, and mortality (Figure 8-1).1 An overview of diuretic dosing in HF is presented in Table 8-2.1
- The optimal treatment strategy for HFPEF remains undefined. However, the following approaches are recommended:
- Control blood pressure. Diuretics, angiotensin-converting enzyme (ACE) inhibitors, angiotensin receptor blockers (ARBs), calcium channel blockers (CCBs), and β-blockers are all reasonable agents to achieve this goal.
- Control heart rate and use warfarin anticoagulation in patients with atrial fibrillation.
- Use diuretics to treat congestive symptoms, being careful to avoid overdiuresis.
- Treat underlying ischemia if present.
- Control blood pressure. Diuretics, angiotensin-converting enzyme (ACE) inhibitors, angiotensin receptor blockers (ARBs), calcium channel blockers (CCBs), and β-blockers are all reasonable agents to achieve this goal.
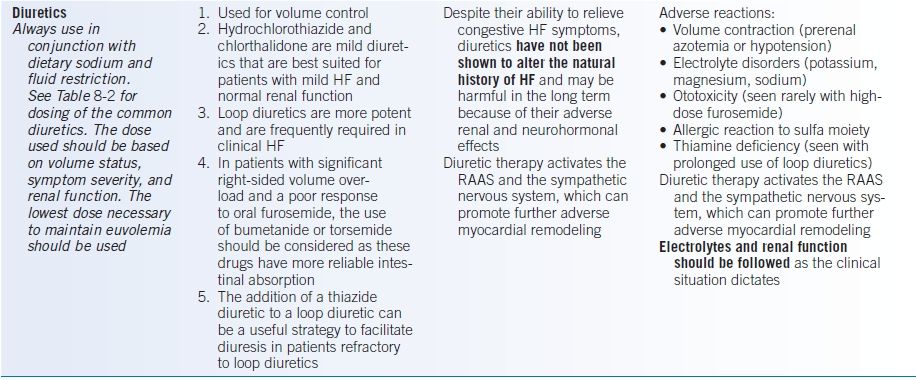
TABLE 8-2 Dosing of Diuretics Commonly Used in Heart Failure
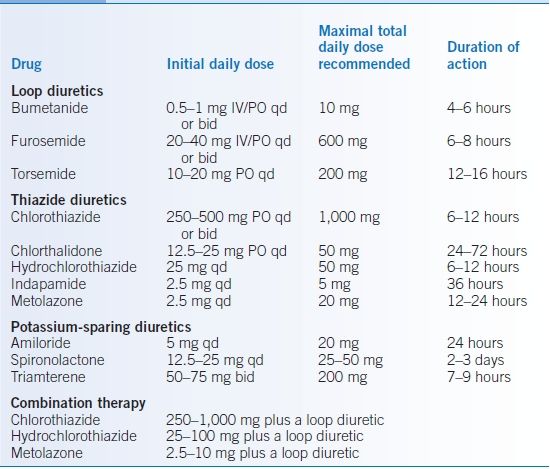
Modified from Yancy CW, Jessup M, Bozkurt B, et al. 2013 ACCF/AHA guideline for the management of heart failure: a report of the American College of Cardiology Foundation/American Heart Association Task Force on practice guidelines. Circulation 2013;128:e240–e327.
Medications
- The pharmacologic management of HFREF is detailed in Table 8-3.5–24
- HFREF is associated with a two- to fourfold increased risk of thromboembolic events, including stroke.
- To date, four randomized controlled trials have failed to show a difference in mortality between placebo versus aspirin versus warfarin in patients with EF <35%. A slight reduction in ischemic stroke has been observed with warfarin, but this is offset by an increased risk of CNS bleeding. The use of aspirin has been associated with increased hospitalization for HF.
- The general consensus is that patients with HFREF should not routinely receive antiplatelet or anticoagulant medications. However, those with atrial fibrillation, LV thrombus, or LV noncompaction should be treated with warfarin. If patients have CAD, aspirin is appropriate.
- In patients with HFREF, the risks and benefits of anticoagulation therapy must be carefully weighed on an individual basis.
TABLE 8-3 Pharmacologic Management of Heart Failure with Reduced Ejection Fraction
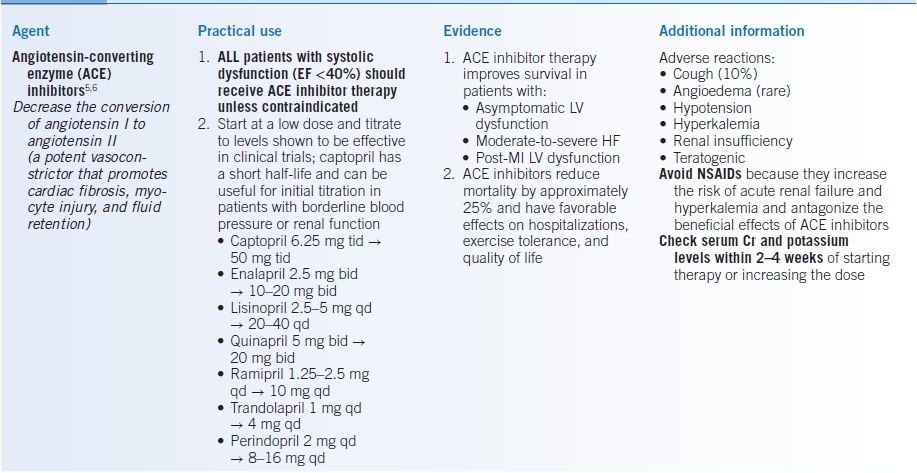
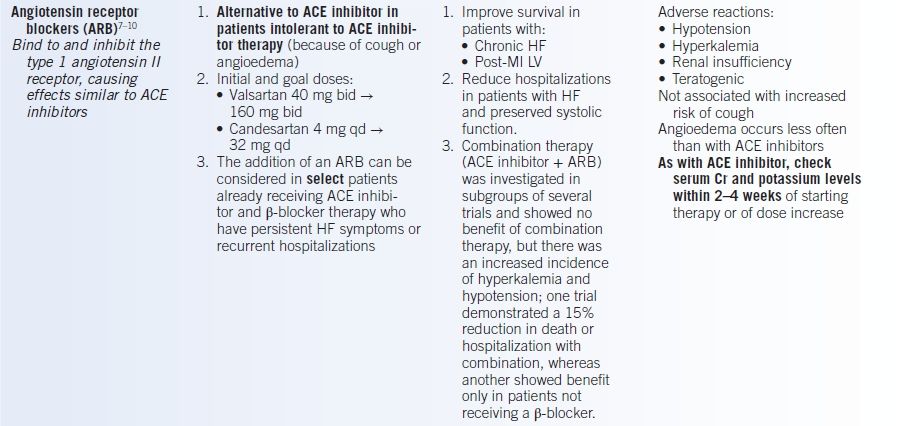
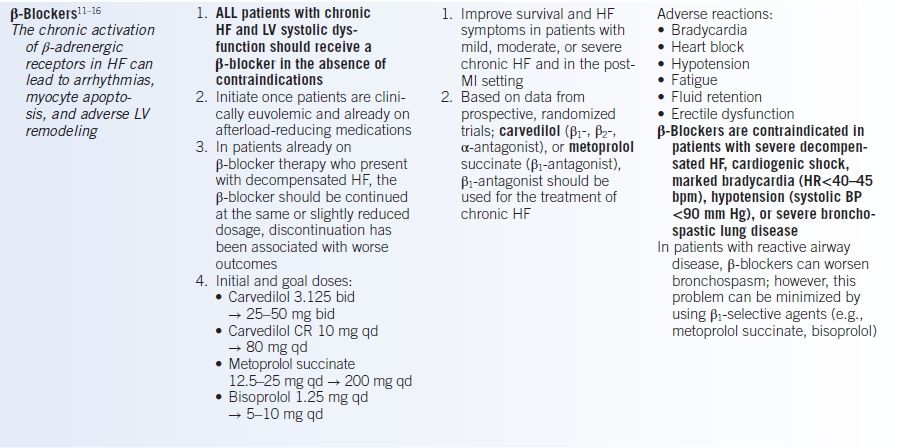
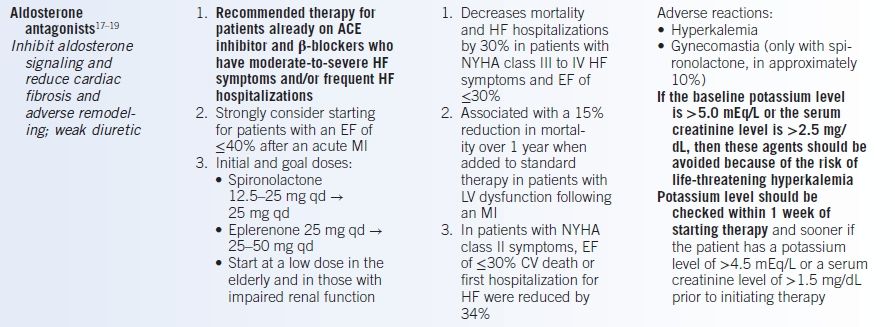
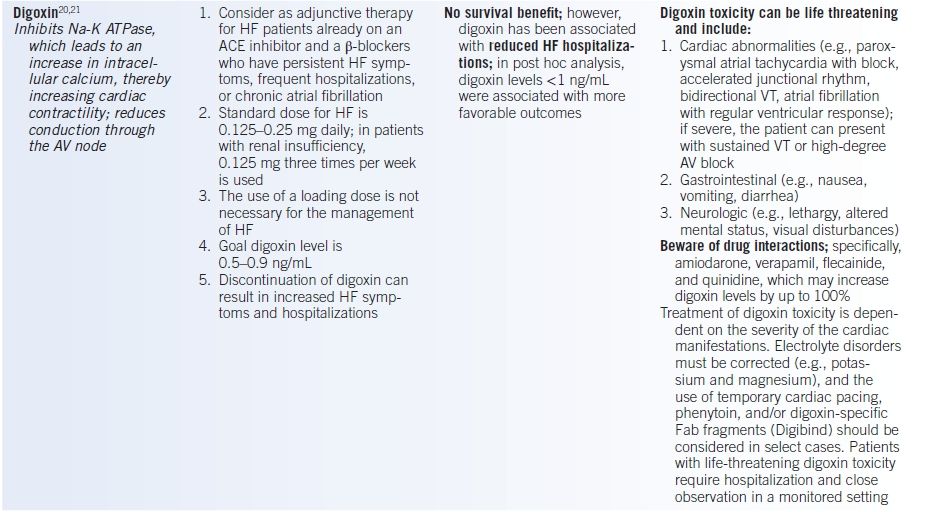
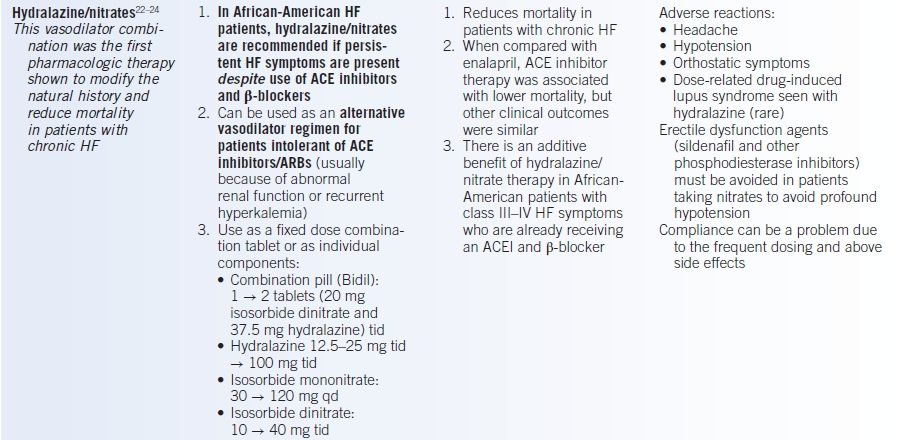
AV, atrioventricular; Cr, creatinine; CV, cardiovascular; EF, ejection fraction; HF, heart failure; LV, left ventricle; MI, myocardial infarction; NYHA, New York Heart Association; RAAS, renin-angiotensin-aldosterone system; VT, ventricular tachycardia.
Other Nonpharmacologic Therapies
- The patient’s nonadherence to medication regimen and diet is a major factor leading to worsened HF symptoms and increased hospitalizations. Therefore, patient education is vital to improve HF outcomes.
- A low-salt diet is necessary to avoid excessive fluid accumulation. In patients with mild-to-moderate HF, sodium intake should be restricted to 2 g/day. Avoidance of foods with high sodium content can help prevent decompensation.
- Patients also need to be educated about fluid intake. For most patients with HF, a 2 L/day maximum fluid intake is appropriate; however, in patients with more severe HF or when hyponatremia is present, more aggressive fluid restriction may be required.
- Patients should obtain (or be provided with) a home scale and maintain a record of daily weights. Increased weight of >2 to 3 pounds from baseline often indicates fluid retention and may warrant adjustment in diuretic dosage.
- Exercise in the form of low-impact aerobic activity is recommended for all HF patients in the absence of contraindications. Physical activity can prevent deconditioning and muscle atrophy, both of which worsen HF prognosis. Heavy weight lifting should be avoided.
- Smoking cessation should be emphasized in patients with current tobacco use; counseling and/or medications should be offered to patients interested in quitting.
- Patients with HF should have yearly influenza vaccination as well as the pneumococcal pneumonia vaccination to minimize the risk of pulmonary infections.
- Implantable cardioverter-defibrillators (ICDs):
- Arrhythmic sudden cardiac death (SCD) accounts for about 50% of all HF-associated deaths.
- ACE inhibitors, β-blockers, and aldosterone antagonists have all been associated with a reduction in SCD; however, despite these therapies, ICDs are associated with improved survival in selected chronic HF patients with reduced systolic function.
- All patients with an EF ≤35%, NYHA class II or III symptoms, and an estimated survival of >1 year should be considered for placement of an ICD for primary prevention of SCD.
- Patients with non-ischemic cardiomyopathy (NICM) should receive ACE inhibitors and β-blockers at optimal doses for at least 3 months prior to implanting an ICD, as many of these patients will have significant improvement in LV function with medical therapy.
- Primary prevention ICD implantation should be delayed by at least 40 days following an acute MI or coronary revascularization.
- Evidence
- MADIT-I and MADIT-II established that ICDs reduce mortality by approximately 1% to 2% per year in selected patients with ischemic cardiomyopathy and an EF of ≤30%.25
- Subsequently, the SCD-HeFT study evaluated patients with either ischemic or nonischemic cardiomyopathy and an EF of ≤35% and found that an ICD improved survival in both patient groups.26
- The DINAMIT study investigated the use of ICD therapy in patients with LV dysfunction within 40 days after acute MI and found no survival benefit with device implantation in this timeframe.27
- Although effective at reducing ventricular ectopy, amiodarone has not been shown to reduce arrhythmic death in patients with HF who have reduced systolic function.
- In general, implantation of a primary prevention ICD is not associated with improved survival during the first 12 to 18 months following insertion.25,26
- MADIT-I and MADIT-II established that ICDs reduce mortality by approximately 1% to 2% per year in selected patients with ischemic cardiomyopathy and an EF of ≤30%.25
- Adverse events
- Complications associated with ICD implantation include pneumothorax/hemothorax, cardiac rupture, bleeding at the generator site, pericarditis, and device infection, but the incidence of major complications is <5% among experienced operators.
- Inappropriate shocks occur in 10% to 25% of patients with ICDs, usually related to device sensing of a supraventricular tachycardia (most commonly atrial fibrillation). Device failure is another possible adverse event.
- Some patients report worse quality of life, especially after receiving an ICD shock.
- Complications associated with ICD implantation include pneumothorax/hemothorax, cardiac rupture, bleeding at the generator site, pericarditis, and device infection, but the incidence of major complications is <5% among experienced operators.
- Arrhythmic sudden cardiac death (SCD) accounts for about 50% of all HF-associated deaths.
- Cardiac resynchronization therapy
- LBBB is present in 20% to 30% of patients with HF. Inter- and intraventricular dyssynchrony produced by LBBB can significantly reduce cardiac efficiency and increase mitral regurgitation.
- Implanting an LV pacemaker lead transvenously via the coronary sinus or by a thoracotomy, in conjunction with an RV pacing lead (i.e., biventricular pacing), can improve ventricular synchrony.
- Cardiac resynchronization therapy (CRT) may be considered for HF patients with an LVEF ≤35%, a QRS duration of >120 msec, and persistent NYHA class II to IV symptoms despite optimal medical therapy. The device can be implanted with or without ICD capabilities.
- Patients with LBBB morphology and QRS duration ≥150 msec are most likely to benefit from CRT. Conversely, the value of CRT in patients without LBBB and QRS duration <150 msec is less certain.
- Evidence: The two largest clinical trials evaluating the efficacy of CRT were COMPANION and CARE-HF.28,29 Both studies demonstrated improved HF symptoms and fewer hospitalizations with CRT. CARE-HF also showed a significant 10% absolute risk reduction in mortality in patients receiving CRT (without ICD).
- Adverse events: CRT devices are associated with the same procedural and infectious complications as described above for ICDs. Adverse events unique to CRT include diaphragmatic stimulation from the LV lead and a higher risk of pericardial tamponade from injury to the coronary sinus. Technical challenges or inadequate cardiac venous anatomy can preclude percutaneous placement of an LV lead. Such patients require a surgical approach for placement of the LV lead.
- LBBB is present in 20% to 30% of patients with HF. Inter- and intraventricular dyssynchrony produced by LBBB can significantly reduce cardiac efficiency and increase mitral regurgitation.
Advanced Chronic Heart Failure (Stage D)
- Definition: Severe HF symptoms (NYHA class IIIb or IV) and/or frequent hospitalizations for HF despite optimal medical therapy.
- Patients with end-stage HF represent about 5% of the total HF population; however, they have an extremely high mortality rate and are frequently hospitalized, mandating close medical attention.
- Potential candidates for heart transplantation and/or an LV assist device (LVAD) should be identified and referred to a HF specialist.
- Patients should be continued on ACE inhibitor/ARB, β-blockers, aldosterone antagonists, and digoxin as blood pressure and renal function allow.
- Congestive symptoms should be managed with diuretics; however, hypotension, renal dysfunction, and diuretic resistance are frequently encountered in these patients.
- Discussions regarding end-of-life care should occur between the patient and provider.
- LVADs/Transplantation
- Advanced HF therapies such as heart transplantation or LVAD implantation should be considered for patients with advanced HF refractory to medical therapy who have few comorbidities. Cardiopulmonary exercise testing can also be useful to identify patients who might benefit from these treatments. A VO2 max of <14 mL O2/kg/minute is predictive of poor outcomes without advanced therapies.
- The use of LVADs for permanent or destination therapy (DT) can be considered for advanced HF patients who are not transplant eligible, do not have other life-limiting organ dysfunction, and have a high risk of HF mortality within the next year (class I, level of evidence B, 2012).30
- ACE inhibitors/ARBs, β-blockers, and aldosterone antagonists can reduce arrhythmias and decrease systemic afterload in LVAD patients and thus should be continued after device implant as renal function, potassium, and blood pressure allow.
- Evidence: In the REMATCH trial, the HeartMate XVE (pulsatile pump) reduced mortality compared to medical therapy in patients with severe HF who were not eligible for cardiac transplantation (REMATCH).31 More recently, the next-generation HeartMate II device (continuous-flow pump) was shown to be superior to the HeartMate XVE, with a 2-year survival rate free of disabling stroke and reoperation to replace the LVAD of 62% versus 7%, respectively.32
- The most common outpatient complications observed in LVAD patients include infection, stroke/cardioembolic events, device thrombosis, gastrointestinal bleeding, ventricular arrhythmias, and recurrent HF (often right HF) with or without multiorgan failure.33,34
- Anticoagulation and antiplatelet therapy is standard for LVAD patients due to the risk of in situ device thrombosis and stroke. The risk of stroke is approximately 10% per patient-year. Goal INR is typically 1.8 to 2.0; however, it is often individualized based on the risk of bleeding and/or thrombotic complications.
- Device-related infections including pump, pump pocket, and driveline infections are serious and can progress to sepsis.
- Device thrombosis is a life-threatening complication that can present as HF and/or hemolysis. The presence of dark urine mandates immediate further evaluation (CBC, UA, LDH, plasma-free hemoglobin, haptoglobin, bilirubin, echocardiogram). Device thrombosis requires urgent transplant or pump exchange.
- Cryptogenic gastrointestinal bleeding is common in LVAD patients, occurring in about 25% of those on HeartMate II support. Close monitoring of INR and hemoglobin is important in the outpatient setting.
- Ventricular arrhythmias remain problematic after LVAD implant. Although tolerated, patients often have palpitations, fatigue, and light-headedness. The use of β-blockers and antiarrhythmic agents can be effective. Most patients already have an ICD in place for prophylaxis although the value of ICDs in LVAD patients is unknown.
- Right HF occurs in about 25% of patients who receive an LVAD leading to an excess of rehospitalizations and mortality. The optimal medical treatment is unknown, but changes in pump speed and/or the use of diuretics, pulmonary vasodilators, or inotropes can be considered.
- Advanced HF therapies such as heart transplantation or LVAD implantation should be considered for patients with advanced HF refractory to medical therapy who have few comorbidities. Cardiopulmonary exercise testing can also be useful to identify patients who might benefit from these treatments. A VO2 max of <14 mL O2/kg/minute is predictive of poor outcomes without advanced therapies.
- Continuous intravenous inotropic therapy can be used as a bridge to transplantation or for symptom palliation in patients who are not transplant or LVAD candidates. However, chronic inotropes have been associated with increased mortality and should therefore be initiated with caution.35 The two inotropic agents currently in use are the β-adrenergic agonist dobutamine and the phosphodiesterase inhibitor milrinone. These medications should be initiated only in consultation with a HF specialist.
- The 1-year mortality for patients with NYHA class III to IV HF symptoms ranges from 50% to 90% depending on patient characteristics. In patients who are not candidates for transplantation or an LVAD, palliative care and hospice should be discussed as mechanisms to provide medical and emotional support during the end-of-life process. Discussions regarding turning off ICDs at the end of life should be undertaken to avoid unnecessary painful events.
Acute Decompensated Heart Failure in the Ambulatory Setting
- In contrast to chronic HF, the management of acute decompensated HF (ADHF) is based more on expert opinion than on clinical trial evidence.
- The primary treatment goals in acute HF syndromes are as follows: (1) to improve patient symptoms, (2) to identify and treat precipitating factors of decompensation, (3) to minimize cardiac and renal injury, and (4) to reduce hospitalization by managing selected cases of mild-to-moderate volume overload in the outpatient setting.
- Identifying and treating potential triggers of an HF exacerbation is critical to improving patient outcomes. The most common causes of decompensation in patients with established HF include the following:
- Medication and dietary noncompliance
- Arrhythmias (particularly atrial fibrillation or ventricular tachycardia (VT))
- Ischemia
- Uncontrolled HTN
- Infections (e.g., pneumonia)
- Substance abuse
- Pulmonary embolism
- Medication and dietary noncompliance
- Upstream management strategies
- Dependence on symptoms (orthopnea) and exam findings (pulmonary rales, peripheral edema, elevated JVP) alone has proven ineffective in averting ADHF hospitalizations. One strategy to improve the sensitivity of detecting early volume overload is through the use of implantable hemodynamic sensors.36
- Several implantable sensors have been developed that monitor parameters such as intracardiac filling pressures or thoracic electrical impedance (a measure of lung fluid content).
- These devices have the potential to reduce HF hospitalizations and improve outpatient medical therapy for HF. Early trials have suggested benefit, but definitive evidence requires further study.
- Dependence on symptoms (orthopnea) and exam findings (pulmonary rales, peripheral edema, elevated JVP) alone has proven ineffective in averting ADHF hospitalizations. One strategy to improve the sensitivity of detecting early volume overload is through the use of implantable hemodynamic sensors.36
- Patients should be considered for hospital admission if they have any of the following:
- Severe symptoms or active myocardial ischemia
- Uncontrolled or new-onset arrhythmias
- Hypoxemia
- Marked tachycardia or bradycardia
- Worsening renal insufficiency (increased creatinine >0.5 to 1 mg/dL from baseline)
- Suspected severe valve disease
- Evidence of drug toxicity
- Severe symptoms or active myocardial ischemia
- For mild HF exacerbations, further testing is not usually indicated. In moderate HF exacerbations, a BMP should be obtained to assess renal function and electrolyte levels.
- In select patients, a CXR, BNP, and/or CBC should be considered to assess HF severity and to evaluate for anemia or infection.
- If ischemia is suspected, an ECG and troponin level should be obtained.
- The treatment of HF exacerbations involves the use of diuretics and vasodilators.
- Table 8-4 provides a rational approach to the outpatient management of HF decompensation.
TABLE 8-4 Outpatient Management of Decompensated Heart Failure (HF)
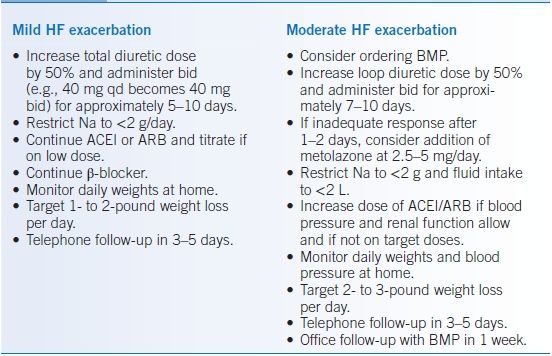
ACEI, angiotensin-converting enzyme inhibitor; ARB, angiotensin receptor blockers; BMP, basic metabolic panel; Na, sodium.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


