Head, Neck, and Endocrine Organs
Atif Ahmed
▪ Questions and Answers
1. This tumor involved the kidney of a 2-year-old boy (Fig. 7.1). The tumor was negative for WT-1 mutations. This tumor will most likely show immunohistochemical staining with:
a. Synaptophysin
b. Myogenin
c. Cytokeratin
d. CD45
e. CD99
View Answer
1. a. The images show a cellular round cell tumor with rosette formation, and it is consistent with neuroblastoma. Although Wilms tumor is common at this age and may rarely have neuroendocrine differentiation, the absence of WT-1 mutations favors neuroblastoma. Neuroblastoma usually stains diffusely with synaptophysin and can be differentiated from Ewing sarcoma, lymphoma, or rhabdomyosarcoma by lack of staining for CD99, CD45, and myogenin, respectively.
Questions 2 and 3:
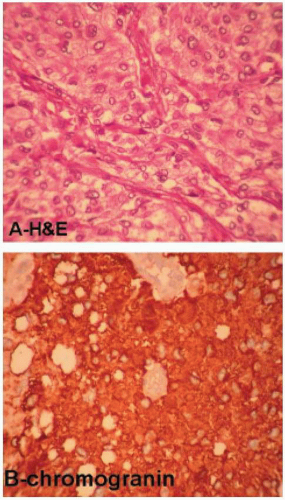
These are sections from a retroperitoneal periaortic abdominal tumor in a 35-year-old man who presented with hypertension (Fig. 7.2).
2. The most likely diag nosis is:
a. Paraganglioma
b. Renin-secreting tumor of the juxtaglomerular apparatus
c. Renal cell carcinoma
d. Hepatocellular carcinoma with neuroendocrine features
e. Carcinoid tumor
View Answer
2. a. The images depict a neuroendocrine tumor with prominent nesting pattern. The clinical presentation, histology, and immunophenotype are characteristics of paraganglioma. Hepatocellular carcinoma may have neuroendocrine features; however, the cytologic features and diffuse positivity of chromogranin do not favor hepatocellular carcinoma. Carcinoid tumor may be confused with paraganglioma but is very rare in the retroperitoneal region. S-100 stain will reveal the characteristic sustentacular cells in paraganglioma. Retroperitoneal paragangliomas occur at an earlier age than head and neck paragangliomas do and are most frequently present at 30 to 40 years of age. Functional paragangliomas cause symptoms related to the production of norepinephrine similar to pheochromocytoma.
3. S-100 immunostain was performed on the tumor in Figure 7.2. Which of the following applies to the cells highlighted by this immunostain (Fig. 7.3)?
a. These cells are of myoepithelial origin.
b. Similar type of cells is normally found in the skin.
c. Their absence in this tumor correlates with more malignant behavior.
d. These cells are also positive for CD21 and CD1a.

View Answer
3. c. These S-100 positive cells are called sustentacular cells. They are of dendritic origin, but they do not stain with CD21 or CD1a. Their presence is diagnostic of paraganglioma, and their absence correlates with malignant behavior. They may be found in some types of carcinoid tumors of the lungs.
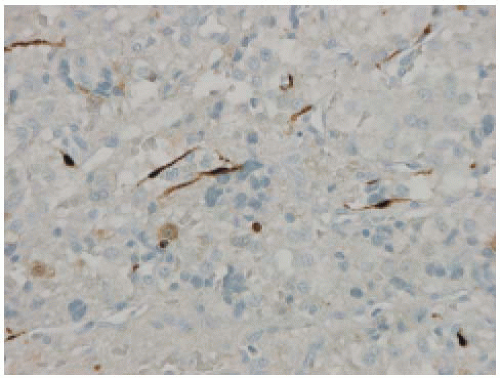 Figure 7.3 |
4. A large posterior mediastinal mass uniformly composed of elements seen in this image (Fig. 7.4) is most likely a:
a. Neurofibroma
b. Schwannoma
c. Ganglioneuroma
d. Gangliocytic paraganglioma
e. Ganglion cell hamartoma
View Answer
4. d. The image shows mature ganglion cells in a background of Schwann cells, thus consistent with ganglioneuroma. Ganglion cells are not uniformly seen in the other entities mentioned in the question, except for ganglion cell choristoma, which is a rare skin tumor. Ganglioneuroma usually presents in the retroperitoneum or mediastinum as an encapsulated mass and is a benign tumor.
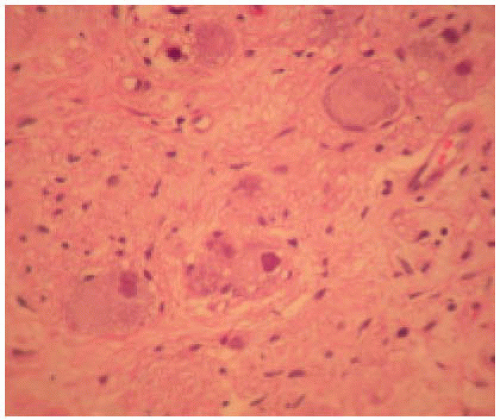 Figure 7.4 |
5. The best treatment of this encapsulated thyroid nodule (Fig. 7.5) is:
a. Enucleation
b. Hormonal therapy
c. Surgical excision with adequate margins
d. Lobectomy
e. Radiotherapy
View Answer
5. d. The image shows the microfollicular pattern of thyroid adenoma. The standard therapy of follicular adenoma is lobectomy. The capsule of the tumor has to be histologically examined to rule out the possibility of follicular carcinoma.
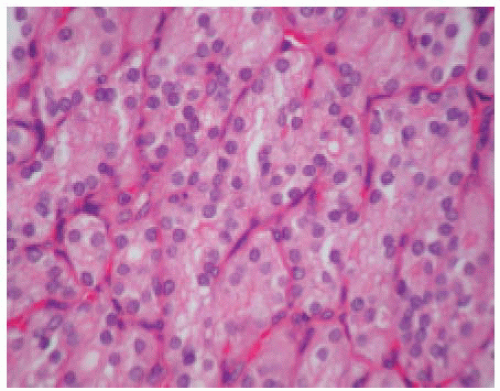 Figure 7.5 |
6. This thyroid lesion (Fig. 7.6) is associated with:
a. Multiple endocrine neoplasia (MEN), type 1
b. MEN type 2
c. RET gene mutations
d. No genetic abnormalities
e. Cystic fibrosis
View Answer
6. c. The image shows the papillary architecture and the characteristic nuclear morphology of papillary thyroid carcinoma (nuclear grooves and clear nuclei). Alteration of the RET oncogene on chromosome 10q11.2 is a characteristic feature of this type of thyroid cancer. Somatic (not germline) rearrangements of RET/PTC genes are found in up to 80% of papillary thyroid carcinoma.
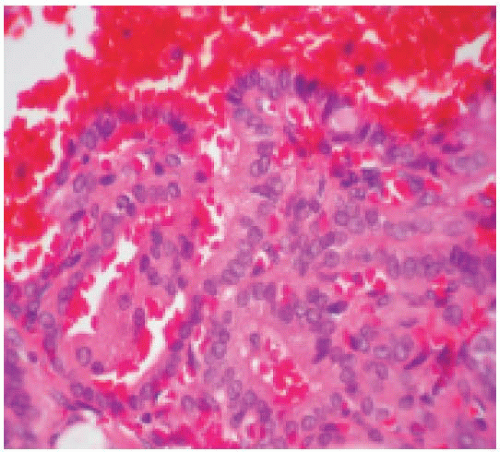 Figure 7.6 |
7. This lesion (Fig. 7.7) in the thyroid is seen mostly in patients with:
a. Multiple endocrine neoplasia (MEN), type 1
b. Cowden syndrome
c. RET gene mutations
d. Hyalinizing trabecular adenoma
e. Goiter
View Answer
7. b. The image shows hyperplastic C cell in interfollicular and intrafollicular locations. Germline RET mutations are found in patients with MEN type 2 and results in C-cell hyperplasia and medullary carcinoma. C-cell hyperplasia is the precursor lesion of medullary thyroid carcinoma.
 Figure 7.7 |
8. A nodule is incidentally found in a hernia sac specimen (Fig. 7.8). The diagnosis is:
a. Adrenal rest
b. Metastatic renal cell carcinoma
c. Clear cell sarcoma
d. Nodular mesothelial hyperplasia
e. Adenomatoid tumor
View Answer
8. a. Ectopic adrenal rests are found in approximately 5% of herniorrhaphy specimens of male children. The circumscription, small size of the nodule, and cytologic features help to differentiate it from metastatic renal cell carcinoma.
9. A tumor that is LEAST likely to occur in patients with multiple endocrine neoplasia (MEN), type 1 is:
a. Pheochromocytoma
b. Thyroid adenoma
c. Pancreatic gastrinoma
d. Appendiceal carcinoid
e. Growth hormone-secreting tumor
View Answer
9. a. Patients with MEN type 1




Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
