Hamartomatous Polyps, Peutz-Jeghers
Amitabh Srivastava, MD
Key Facts
Terminology
Peutz-Jeghers polyposis syndrome is characterized by mucocutaneous pigmentation, hamartomatous polyposis, and increased risk of cancer
Etiology/Pathogenesis
Germline mutation in LKB1/STK11 gene on chromosome 19p13.3 present in 50-70% of patients
Clinical Issues
Pigmented macules
Abdominal pain, anemia, hematochezia
Increased risk of cancer of gastrointestinal tract, pancreas, and breast
Similar polyps may occur in sporadic setting
Removal of small polyps by polypectomy; surgical intervention for obstruction or cancer
Macroscopic Features
Jejunum and ileum most common sites
Variable size; larger polyps are pedunculated and predispose to intussusception
Microscopic Pathology
Papillary architecture with arborizing compact bundles of smooth muscle
Smooth muscle separates epithelial component into distinct lobular configuration
Mucocutaneous lesions
Other distinctive tumors in PJPS
Ovarian sex cord tumor with annular tubules
Testicular large cell calcifying Sertoli cell tumor
Testicular intratubular large cell hyalinizing Sertoli cell tumor
Adenoma malignum of cervix
 Pedunculated Peutz-Jeghers polyps, like the ones illustrated here, may present with small intestinal obstruction when they undergo intussusception. |
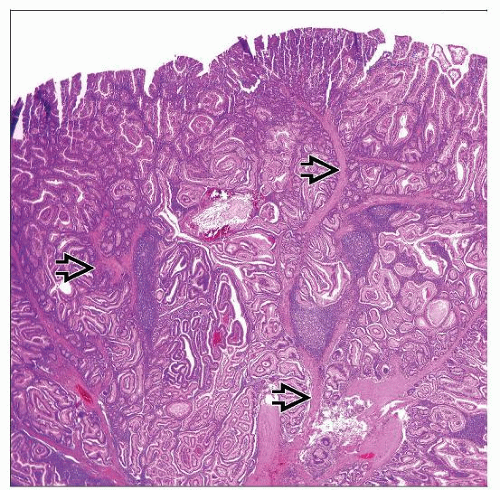 Histologically, Peutz-Jeghers polyps are characterized by tree-like arborizing strands of smooth muscle  that separate the epithelial component into lobules. that separate the epithelial component into lobules. |
TERMINOLOGY
Abbreviations
Peutz-Jeghers polyp (PJP)
Peutz-Jeghers polyposis syndrome (PJPS)
Definitions
PJP may occur sporadically or as part of inherited polyposis syndrome
PJPS is characterized by
Pigmented melanotic lesions around mouth, lips, and oral cavity
Hamartomatous polyposis involving gastrointestinal tract
Increased risk of cancer of GI tract, pancreas, and breast
ETIOLOGY/PATHOGENESIS
Genetics of PJPS
Autosomal dominant pattern of inheritance
Germline mutation in STK11 (LKB1) gene on chromosome 19p13.3
STK11 gene encodes protein that localizes to nucleus and cytoplasm and is postulated to be involved in
Cell polarity
Chromatin remodeling
Cell cycle arrest
Wnt signaling
About 50-70% of patients with PJP have identifiable germline mutations in STK11 gene
Mutations can be identified by direct sequencing or multiple ligation probe-dependent amplification
Mutations in LKB1/STK11 lead to dysregulation of mTOR pathway
More severe phenotype with truncating mutations
CLINICAL ISSUES
Epidemiology
Incidence
Exact incidence uncertain; estimates range from 1/25,000 to 1/300,000
Age
2/3 of PJPS patients present in 2nd to 3rd decade of life
About 1/3 present in 1st decade
Presentation
Pigmented melanotic lesions
In infancy and early childhood
Lips most common site (> 95%)
Buccal mucosa involved in ˜ 80% of patients
Other sites include
Area around mouth and nose
Hands and feet
Pigmented spots may fade with age
Abdominal pain
Obstruction
Intussusception
Anemia
Due to occult GI bleeding
Hematochezia
Hematemesis
In patients with gastric and duodenal polyposis
Prolapse of rectal polyps
Other associated anomalies
Polyps may also be present in
Bladder
Renal pelvis
Bronchus
Nose
Gallbladder
Skeletal anomalies
Club foot
Scoliosis
Neoplastic lesions associated with PJPS
Colon cancer
Pancreatic cancer
Small intestinal and gastric cancer
Breast cancer
Distinctive tumors of genital tract
Sex cord tumor with annular tubules (SCTAT) of ovary
Large cell calcifying Sertoli tumor of testis
Adenoma malignum of cervix



