(1)
Department of Pathology, Radboud University Nijmegen Medical Center, Nijmegen, The Netherlands
Keywords
JawGiant Cell Lesions8.1 Introduction
Central giant cell granuloma , cherubism and aneurysmal bone are defined by the presence of osteoclastic giant cells and are taken together because of this common histological feature. The first two entities are confined to the jaws, the third may occur at other body sites as well [1].
8.2 Central Giant Cell Granuloma
Central giant cell granuloma is a jaw lesion characterized by the presence of hemorrhages and osteoclastic giant cells. In older literature, the term giant cell reparative granuloma is occasionally employed due to a presumed traumatic etiology, a presumption that has not withstood the test of time. The lesion mostly is seen before the age of 30 and involves the mandible more often than the maxilla. Multiple giant cell lesions may occur in association with Noonan’s syndrome as well as with neurofibromatosis [2, 3]. Lesions show a broad variation in size, from small to large and destructive (Figs. 8.1, 8.2 and 8.3).

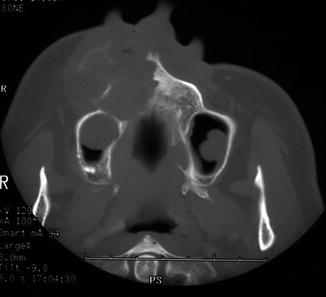
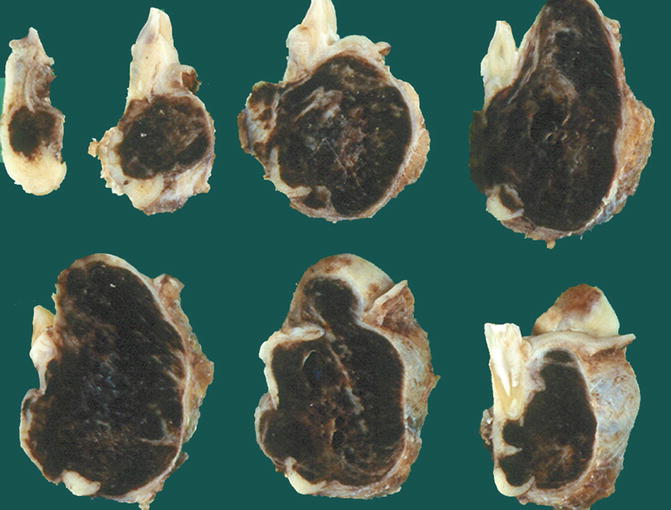
Fig. 8.1
Radiograph of a small central giant cell granuloma, visible as a radiolucent lesion in the mandibular midline
Fig. 8.2
Radiograph of a large maxillary central giant cell granuloma showing extensive loss of maxillary bone and bulging into the buccal soft tissues
Fig. 8.3
Gross specimen of mandibular central giant cell granuloma. Due to hemorrhage, the tissue is deep brown. Bone destruction is apparent but a fibrous capsule separates the lesion from the surrounding soft tissues
Central giant cell granuloma shows osteoclast-like giant cells lying in a fibroblastic background tissue. The giant cells mostly cluster in areas of hemorrhage but they also may lie more dispersed among the lesion (Figs. 8.4, 8.5, 8.6 and 8.7). Mitotic figures may be encountered but are usually not numerous and not atypical (Fig. 8.8). Bone formation, if present, usually is confined to the periphery of the lesion or occurs in less cellular fibrous septa that may divide the lesion in separate foci; they do not form a part of the lesion but represent metaplastic stroma changes (Figs. 8.9 and 8.10).
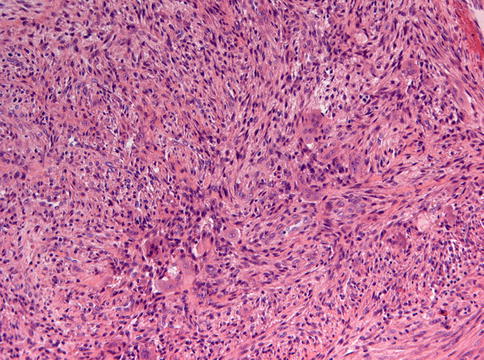
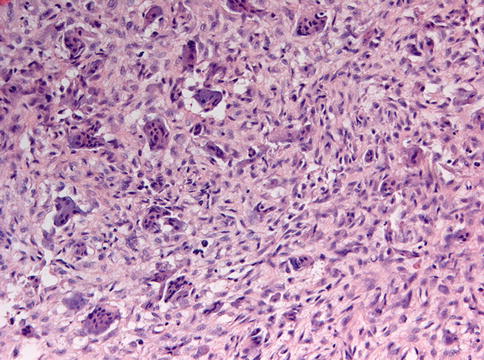

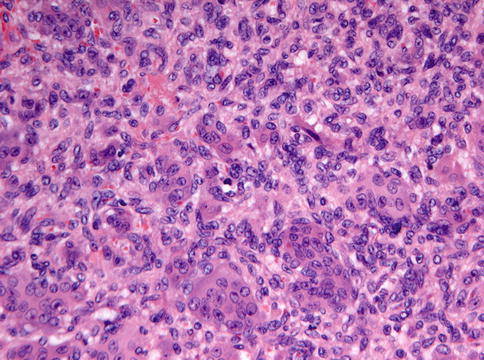
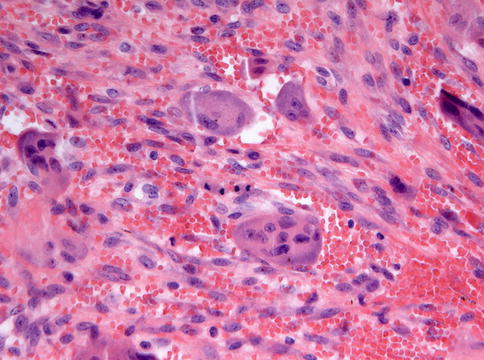

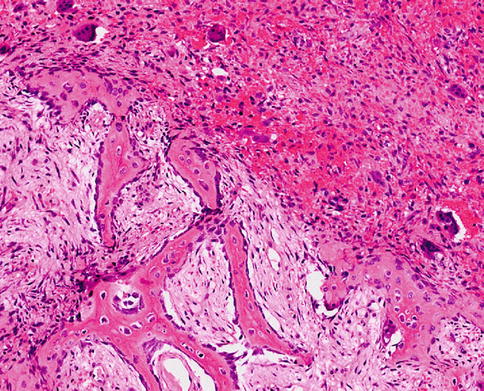
Fig. 8.4
Low power view of central giant cell granuloma, showing fibrocellular background with foci of giant cells
Fig. 8.5
Giant cell granuloma with giant cells lying less focally but more dispersed in a fibrocellular background
Fig. 8.6
Central giant cell granuloma with giant cells clustering in areas of hemorrhage
Fig. 8.7
Central giant cell granuloma with a more uniform appearance, homogeneous cell-rich background tissue with dispersed giant cells and occasionally foci of extravasated erythrocytes
Fig. 8.8
Central giant cell granuloma in which some mitotic figures are encountered
Fig. 8.9
Low power view of central giant cell granuloma to show that bone formation is mainly restricted to fibrous septa connected with the periosteal layer present at the periphery of the lesion and not within the lesional tissue proper
Fig. 8.10
At higher magnification, it is apparent that bone matrix ix not produced by the lesional cells but by a rim of osteoblasts that are separate from the more epitheloid lesional cells
Lesions with an histologic appearance identical to central giant cell granuloma may occur in the gingiva and are called giant cell epulis. Sometimes, lesions combine the appearance of giant cell granuloma with ossifying fibroma (Figs. 8.11, 8.12 and 8.13).
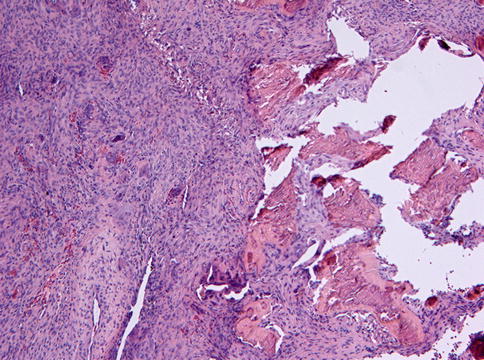
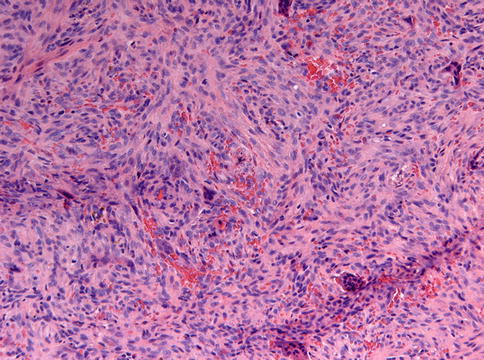
Fig. 8.11
Low power view of lesion that combines features of giant cell granulom (left side) with ossifying fibroma (right side)
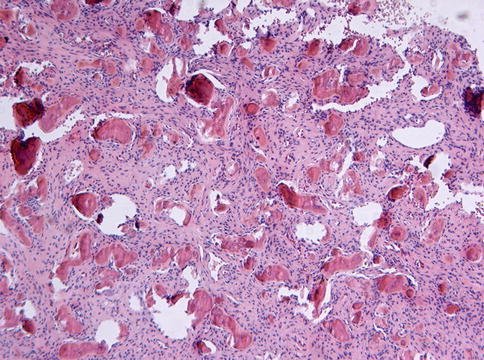
Fig. 8.13




Higher magnification of Fig. 8.11 to illustrate the giant cell granuloma component
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
