Chapter 15 Gastroenterology
Antacids: Buffers





Pharmacokinetics
 Calcium, magnesium, and aluminum are typically poorly absorbed. However, patients with impaired renal function can have accumulation of these cations.
Calcium, magnesium, and aluminum are typically poorly absorbed. However, patients with impaired renal function can have accumulation of these cations.




Side Effects

Ca2+-Containing Buffers
 Hypercalcemia (at high doses): These agents may lead to formation of calculi (milk alkali syndrome). Calculi are solid formations, typically consisting of minerals, which precipitate in organs such as the kidney and obstruct ducts.
Hypercalcemia (at high doses): These agents may lead to formation of calculi (milk alkali syndrome). Calculi are solid formations, typically consisting of minerals, which precipitate in organs such as the kidney and obstruct ducts.



Important Notes
 Although these agents act locally in the stomach, they are not devoid of systemic adverse effects, particularly at higher doses or with chronic use.
Although these agents act locally in the stomach, they are not devoid of systemic adverse effects, particularly at higher doses or with chronic use.




FYI
 Although the agents in this class have traditionally been referred to as antacids, the term antacid has much wider use and applies to each of the many classes of drugs that reduce acid secretion. The more appropriate term for the agents in this class is buffer, as this describes their mechanism and distinguishes them from other classes.
Although the agents in this class have traditionally been referred to as antacids, the term antacid has much wider use and applies to each of the many classes of drugs that reduce acid secretion. The more appropriate term for the agents in this class is buffer, as this describes their mechanism and distinguishes them from other classes.H2 Antagonists


Moa (Mechanism of Action)
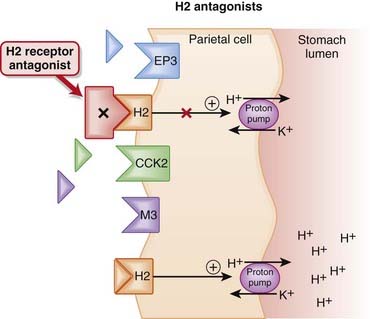
 The amount of gastric acid is largely determined by the secretion of protons (H+) by parietal cells in the stomach, as well as volume of stomach contents.
The amount of gastric acid is largely determined by the secretion of protons (H+) by parietal cells in the stomach, as well as volume of stomach contents.
 The H2 receptor on parietal cells mediates both the basal and meal-stimulated release of acid. The binding of histamine to the H2 receptor stimulates the proton (H+/K+ ATPase) pump via the second messenger cyclic adenosine monophosphate (cAMP) (Figure 15-1).
The H2 receptor on parietal cells mediates both the basal and meal-stimulated release of acid. The binding of histamine to the H2 receptor stimulates the proton (H+/K+ ATPase) pump via the second messenger cyclic adenosine monophosphate (cAMP) (Figure 15-1).



Pharmacokinetics
 All the H2 antagonists are available in oral formulations. Intravenous and intramuscular formulations of cimetidine, ranitidine, and famotidine are also available.
All the H2 antagonists are available in oral formulations. Intravenous and intramuscular formulations of cimetidine, ranitidine, and famotidine are also available.












Important Notes
 The H2 antagonists are considered to be less effective than the more expensive proton pump inhibitors (PPIs). However, it is important to note that the H2 antagonists are able to reduce daily acid secretion by about 60% to 70%.
The H2 antagonists are considered to be less effective than the more expensive proton pump inhibitors (PPIs). However, it is important to note that the H2 antagonists are able to reduce daily acid secretion by about 60% to 70%.


Evidence

Versus Other Agents for Endoscopy Negative Reflux Disease
 The same 2006 Cochrane review found that PPIs were more efficacious at achieving heartburn remission compared with H2 antagonists (three trials, RR 0.78) and compared with prokinetics (one trial, RR 0.72). Endoscopy-negative reflux disease is simply GERD without any evidence of histologic changes on endoscopic examination.
The same 2006 Cochrane review found that PPIs were more efficacious at achieving heartburn remission compared with H2 antagonists (three trials, RR 0.78) and compared with prokinetics (one trial, RR 0.72). Endoscopy-negative reflux disease is simply GERD without any evidence of histologic changes on endoscopic examination.


Proton Pump Inhibitors (PPIs)


Moa (Mechanism of Action)
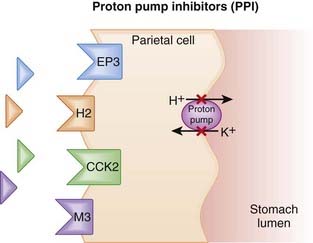
 The amount of gastric acid is largely determined by the secretion of protons (H+) by parietal cells in the stomach, as well as the volume of stomach contents.
The amount of gastric acid is largely determined by the secretion of protons (H+) by parietal cells in the stomach, as well as the volume of stomach contents. In the parietal cell, the proton pump, H+/K+ ATPase, creates an ion gradient by pumping H+ into the lumen of the stomach. The pump is key to creating the acidic environment of the stomach (pH <1) while maintaining a relatively normal intracellular pH (approximately 7.3) (Figure 15-2).
In the parietal cell, the proton pump, H+/K+ ATPase, creates an ion gradient by pumping H+ into the lumen of the stomach. The pump is key to creating the acidic environment of the stomach (pH <1) while maintaining a relatively normal intracellular pH (approximately 7.3) (Figure 15-2).


Pharmacokinetics
 Although they act on cells in the stomach, PPIs must be absorbed into the systemic circulation from the small intestine. It is from the systemic circulation that they reach the parietal cells of the stomach.
Although they act on cells in the stomach, PPIs must be absorbed into the systemic circulation from the small intestine. It is from the systemic circulation that they reach the parietal cells of the stomach.











Side Effects


Less Common
 Hypergastrinemia: Gastrin levels become elevated because of the body’s response to chronic gastric acid suppression. This may lead to rebound hypersecretion of gastric acid if the PPI is stopped. There is also concern over the chronic effects of hypergastrinemia, including development of gastric tumors.
Hypergastrinemia: Gastrin levels become elevated because of the body’s response to chronic gastric acid suppression. This may lead to rebound hypersecretion of gastric acid if the PPI is stopped. There is also concern over the chronic effects of hypergastrinemia, including development of gastric tumors.Important Notes
 Of all agents used to treat hyperacidity, PPIs are the most effective at reducing daily acid secretion, capable of reducing acid (basal and stimulated) by 80% to 95%. H2 antagonists are able to achieve a 60% to 70% reduction in acid.
Of all agents used to treat hyperacidity, PPIs are the most effective at reducing daily acid secretion, capable of reducing acid (basal and stimulated) by 80% to 95%. H2 antagonists are able to achieve a 60% to 70% reduction in acid.
 PPIs are often prescribed in combination with other GI drugs and antibiotics for eradication of H. pylori. By increasing intragastric pH, PPIs appear to enhance the antimicrobial activity of these agents. PPIs may also have a minor antimicrobial effect. Some of the more common combinations are listed in Table 15-1.
PPIs are often prescribed in combination with other GI drugs and antibiotics for eradication of H. pylori. By increasing intragastric pH, PPIs appear to enhance the antimicrobial activity of these agents. PPIs may also have a minor antimicrobial effect. Some of the more common combinations are listed in Table 15-1.TABLE 15-1 Combination Therapy for H. pylori Eradication
| Proton Pump Inhibitors | Other Agents | |
|---|---|---|
| Lansoprazole | Clarithromycin | Amoxicillin |
| Omeprazole | Clarithromycin | Metronidazole |
| Pantoprazole | Metronidazole | |
| Rabeprazole | Bismuth subsalicylate | Tetracycline |



Evidence

Versus Other Agents for Endoscopy Negative Reflux Disease
 The same 2006 Cochrane review found that PPIs were more efficacious at achieving heartburn remission compared with H2 antagonists (three trials, RR 0.78) and compared with prokinetics (one trial, RR 0.72). Endoscopy-negative reflux disease is simply GERD without any evidence of histologic changes on endoscopic examination.
The same 2006 Cochrane review found that PPIs were more efficacious at achieving heartburn remission compared with H2 antagonists (three trials, RR 0.78) and compared with prokinetics (one trial, RR 0.72). Endoscopy-negative reflux disease is simply GERD without any evidence of histologic changes on endoscopic examination.Versus H2 Antagonists for Acute Bleeding from Peptic Ulcer
 A 2006 Cochrane review (24 studies, N = 4373 patients) found no difference in mortality between PPIs and controls but did find that PPIs reduced rebleeding (incidence of 10.6% for PPI versus 17.3% control) and surgery (6.1% versus 9.3%, respectively) versus control. No benefit was seen for PPIs versus H2 antagonists with regard to surgery.
A 2006 Cochrane review (24 studies, N = 4373 patients) found no difference in mortality between PPIs and controls but did find that PPIs reduced rebleeding (incidence of 10.6% for PPI versus 17.3% control) and surgery (6.1% versus 9.3%, respectively) versus control. No benefit was seen for PPIs versus H2 antagonists with regard to surgery.
Gastrointestinal Cytoprotectants


Moa (Mechanism of Action)
Prostaglandin Analogue
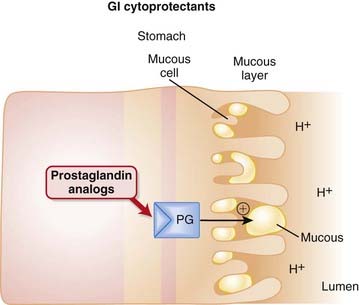
 Protection of the mucosal lining of the stomach can be achieved in two ways: by increasing gastric pH or by enhancing the mucosal barrier that protects the stomach.
Protection of the mucosal lining of the stomach can be achieved in two ways: by increasing gastric pH or by enhancing the mucosal barrier that protects the stomach.
 Endogenous PGE2 acts as an agonist at EP3 receptors on parietal cells and reduces activity of the proton pump, thereby reducing secretion of gastric acid (Figure 15-3).
Endogenous PGE2 acts as an agonist at EP3 receptors on parietal cells and reduces activity of the proton pump, thereby reducing secretion of gastric acid (Figure 15-3).


 Therefore a PGE1 analogue such as misoprostol is typically given as an adjunct in patients undergoing NSAID therapy, for the purpose of substituting for the PGE lost with NSAID use (Figure 15-4).
Therefore a PGE1 analogue such as misoprostol is typically given as an adjunct in patients undergoing NSAID therapy, for the purpose of substituting for the PGE lost with NSAID use (Figure 15-4).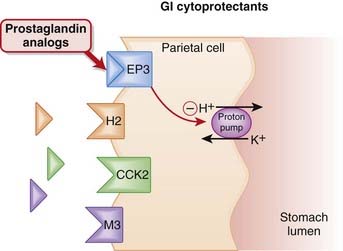
Sucralfate
 Sucralfate is a complex of sucrose and aluminum hydroxide that forms a viscous paste in aqueous acidic media. This negatively charged paste binds to positively charged proteins in the ulcer, forming a direct protective barrier for up to 6 hours.
Sucralfate is a complex of sucrose and aluminum hydroxide that forms a viscous paste in aqueous acidic media. This negatively charged paste binds to positively charged proteins in the ulcer, forming a direct protective barrier for up to 6 hours.





