Patient Story
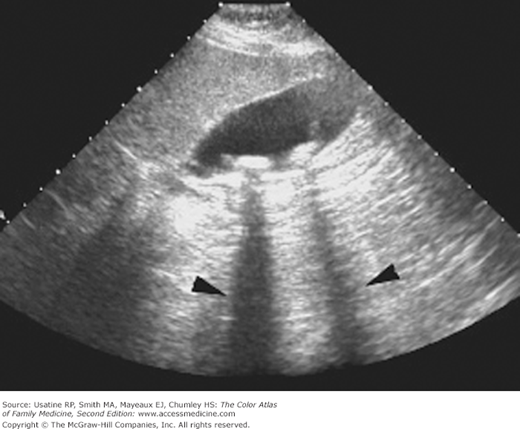
A 44-year-old woman reports frequent episodes of severe pain in the mid and upper right-side of her abdomen that usually occurs shortly after her evening meal and sometimes at night. She is obese, but otherwise healthy. The pain lasts for several hours and is steady and often causes vomiting. On physical examination she complains of slight tenderness in the right upper quadrant (RUQ). An ultrasound confirms the presence of gallstones (Figure 62-1).
Introduction
Gallstones are concretions (inorganic masses), usually composed of cholesterol, that form in the gallbladder or bile duct. They are formed by concretion (joining together of adjacent parts and hardening) or accretion (growth by addition or adherence of parts normally separated) of normal and/or abnormal bile constituents.
Epidemiology
- Based on autopsy data, 20% of women and 8% of men have gallstones.1
- Approximately 20 million people in the United States are affected, with 1 million new cases each year.1
- In a Swedish incidence study of 621 randomly selected individuals ages 35 to 85 years, 42 (8.3%) of the 503 subjects available at 5 years developed gallstones; this yielded an incidence for newly developed gallstones of 1.39 per 100 person-years.2
- Among pregnant women, 5% to 12% have gallstones and 20% to 30% have gallbladder sludge (thick mucous material containing cholesterol crystals and mucin thread or mucous gels). Gallbladder sludge is a possible precursor form of gallstone disease.1
- Patients with asymptomatic gallstones have a 1% to 2% risk per year of developing symptoms or complications of gallstones. Based on data primarily for men, this will occur in 10% by 5 years, 15% by 10 years, and 18% by 15 years following diagnosis.1
- Gallstone disease is responsible for approximately 10,000 deaths per year in the United States. Most (7000) of these deaths are attributable to acute gallstone complications (e.g., cholecystitis, pancreatitis, cholangitis).3
- Although gallbladder cancers most often occur in the setting of stones (91% of 34 patients with gallbladder cancer in one study),4 gallbladder cancer is rare. An incidence rate of 0.28% for incidental gallbladder carcinoma was reported in a Swiss database study of a population of more than 30,000 patients undergoing laparoscopic cholecystectomy.5
Etiology and Pathophysiology
- There are two types of gallstones: cholesterol stones (80%) and pigmented stones (primarily calcium bilirubinate, 20%).
- The solute components of bile include bile acids (80%), lecithin and other phospholipids (16%), and unesterified cholesterol (4%).1 Cholesterol gallstones form when there is excess cholesterol or an abnormal ratio of cholesterol, bile acids, and lecithin.
- Excess biliary cholesterol can occur from a secondary increase in secretion of cholesterol caused by obesity, high cholesterol diet, clofibrate therapy, or a genetic predisposition to increased hydroxymethylglutaryl-coenzyme A reductase.
- The excess cholesterol becomes supersaturated and can precipitate out of solution in a process called nucleation, forming solid cholesterol monohydrate crystals that can become trapped in gallbladder mucus, producing sludge, and/or grow and aggregate to form cholesterol gallstones.
- Gallbladder hypomotility is a predisposing and possibly necessary factor in stone formation because of the failure to completely empty supersaturated or crystal-containing bile.1 Situations associated with hypomotility include pregnancy, prolonged parenteral nutrition, surgery, burns, and use of oral contraceptives or estrogen therapy.
- Pigmented stones occur when increasing amounts of unconjugated bilirubin in bile precipitate to form stones. Bilirubin, a yellow pigment derived from the breakdown of heme, is actively secreted into bile by liver cells. In situations of high heme turnover, such as chronic hemolytic states (e.g., sickle cell anemia), calcium bilirubinate can crystallize from solution and form stones.
- Chronic gallstones may cause progressive fibrosis of the gallbladder wall and loss of function.
Risk Factors
- Genetic mutations can result in reduction of bile acids and lecithin that predispose some patients to stone formation. A high prevalence of gallstones is found in first-degree relatives of patients with gallstones and among Native Americans, Chilean Indians, and Chilean Hispanics.1
- In a case-control study, the prevalence of gallstones was 28.6% in first-degree relatives of subjects with gallstones versus 12.4% in first-degree relatives of subjects without gallstones (relative risk [RR] 1.80, 95% confidence interval [CI] 1.29 to 2.63).3
- Other risk factors for gallstones include rapid weight loss (10% to 20% of these patients form stones),1 increasing age, liver or ileal disease, and cystic fibrosis.
Diagnosis
- Symptoms of gallstones are caused from inflammation or obstruction as stones migrate into the cystic or common bile duct (CBD).
- Biliary colic is a steady, severe pain or ache, usually of sudden onset, located in the epigastrium or RUQ. Pain episodes last between 30 minutes and 5 hours and may radiate to the interscapular area, right scapula, or right shoulder.
- Gallstone-related pain may be precipitated by a fatty meal, a regular meal or a large meal followed by a prolonged fast.
- Pain is recurrent and often nocturnal.
- Biliary colic is a steady, severe pain or ache, usually of sudden onset, located in the epigastrium or RUQ. Pain episodes last between 30 minutes and 5 hours and may radiate to the interscapular area, right scapula, or right shoulder.
- RUQ tenderness may be elicited on physical examination.
- Nausea and vomiting are common.
- Accompanying fever and chills suggests a complication of gallstones. Complications are more common in patients with a calcified gallbladder or in those who have had a previous episode of acute cholecystitis.1
- No laboratory testing is usually indicated as the results are usually normal. However, an elevated γ-glutamyl transpeptidase suggests a CBD stone. In a study of patients with acute calculous gallbladder disease, investigators found a 1-in-3 chance of CBD stones when the γ-glutamyl transpeptidase level was above 90 U/L and a 1-in-30 chance when the level was less than 90 U/L.6
- Ultrasound is the diagnostic test of choice and is 95% accurate for stones as small as 2 mm in diameter (Figure 62-1).1 Shadowing, a discrete acoustic shadow caused by the absorption and reflection of sound by the stone that changes with patient positioning, is an important diagnostic feature that is shown in Figures 62-1 and 62-2.
- In one study, high-resolution ultrasound was more accurate than endoscopic ultrasonography or CT in differentiating benign disease from malignancy in cases with gallbladder polypoid lesions.7
- Gallstones may be seen on plain film, but only calcified stones are seen (Figures 62-3 and 62-4). This includes only 10% to 15% of cholesterol stones and 50% of pigmented stones.1 Stones may be single or multiple and the gallbladder wall may be calcified (referred to as a Porcelain gallbladder), indicating severe chronic cholecystitis or adenocarcinoma.
- CT is less sensitive and more expensive than ultrasound for the detection of gallstones (Figures 62-5 and 62-6). However, CT can detect both radiopaque stones and radiolucent stones.
- An oral cholecystogram can be used to assess cystic duct patency and emptying function. This test has largely been replaced by gallbladder ultrasound.
- Radioisotope scans (e.g., technetium [Tc]-99m hepatoiminodiacetic acid [HIDA]) can be used to confirm acute cholecystitis (nonvisualizing gallbladder) and can be useful in evaluating functional abnormalities.
- Endoscopic retrograde cholangiopancreatography is used for imaging bile ducts. Stones in bile appear as filling defects in the opacified ducts. Endoscopic retrograde cholangiopancreatography is usually performed in conjunction with endoscopic retrograde sphincterotomy and gallstone extraction.



