Focal Segmental Glomerulosclerosis, Secondary
A. Brad Farris, III, MD
Key Facts
Terminology
FSGS secondary to imbalance of glomerula-functional capacity and demand
Etiology/Pathogenesis
Adaptive structural-functional response
Reduced nephron mass: Oligomeganephronia, reflux nephropathy, renal agenesis/dysplasia/ablation/necrosis, advanced renal disease
Normal nephron mass: HTN, obesity, atheroemboli/vaso-occlusion, sickle cell anemia, congenital heart disease, drugs (anabolic steroids, calcineurin inhibitors)
Glomerular HTN
Clinical Issues
Proteinuria and systemic HTN
Microscopic Pathology
Glomerulomegaly
FSGS in perihilar distribution
Compensatory tubular hypertrophy
Often arteriolar hyalinosis, arteriosclerosis
IF: Most notable for segmental IgM and C3
EM: Segmental podocyte foot process effacement (FPE)
Increased thickness of otherwise normal GBM
Top Differential Diagnoses
Primary FSGS
Segmental scars from GN
Diagnostic Checklist
Routinely assess glomerular size in biopsies
Normal is < 50% of diameter of 40x field
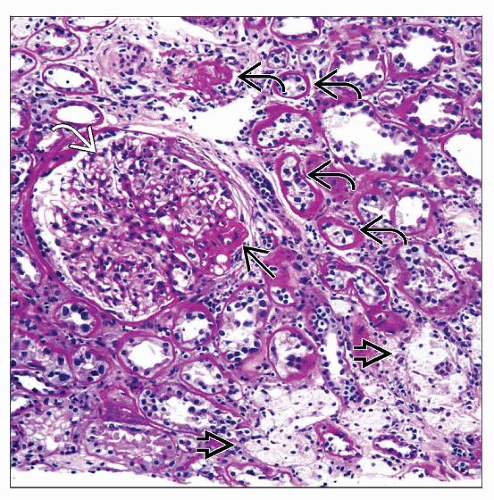 Secondary FSGS is often manifested by glomerulomegaly  and a perihilar distribution of the glomerular adhesions and a perihilar distribution of the glomerular adhesions  . This case also shows interstitial foam cells . This case also shows interstitial foam cells  and tubular atrophy and tubular atrophy  . . |
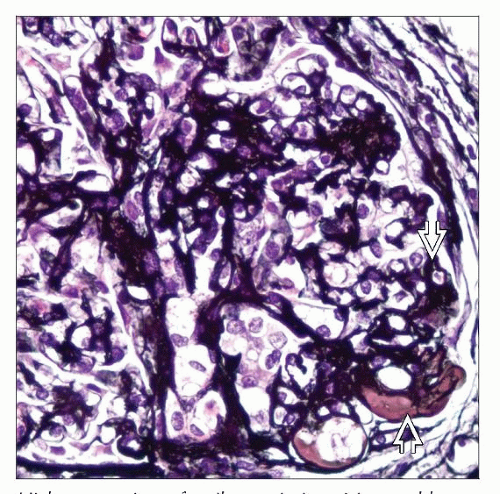 High-power view of a silver stain in a 21-year-old man with nephrotic syndrome and perihilar segmental GS shows that intracapillary hyaline  is present in the segmental sclerosis lesion. is present in the segmental sclerosis lesion. |
TERMINOLOGY
Abbreviations
Secondary focal segmental glomerulosclerosis (2° FSGS)
Definitions
“Primary” and “secondary” FSGS terminology confusing since specific causal mechanisms are being identified in both
Here, 2° FSGS is defined as FSGS that arises as maladaptive response to loss of nephrons or increased demand, probably due to increased filtration/perfusion of glomeruli and podocyte stress
ETIOLOGY/PATHOGENESIS
Adaptive Structural-Functional Response
Imbalance between glomerular capacity and metabolic demands
Thought to act through glomerular hypertension (HTN), increased filtration, and podocyte stress
↑ glomerular capillary pressures and flow rates
Arises from several pathways
Failure to develop normal number of glomeruli
Unilateral renal agenesis, dysplasia, oligomeganephronia, and other congenital renal developmental diseases
Acquired disease that causes ↓ of functional nephrons
Sequelae of chronic renal disease of any etiology that destroys nephrons: Final common pathway
Reflux nephropathy, Alport syndrome, HTN, cortical necrosis, and virtually any other chronic renal disease
Normal number of glomeruli but increased “demand”
Obesity, body builders, anabolic steroids, possibly HTN
Specific Mechanisms
Obesity-related glomerulopathy (ORG)
Receptor for advanced glycation end products (RAGE) may mediate obesity-associated renal injury
RAGE may also be important to diabetes, doxorubicin-induced nephropathy, HTN, lupus nephritis, ischemic renal injury, and renal amyloidosis
RAGE antagonism may be useful in treating chronic kidney disease
Calcineurin inhibitors (CNIs)
Arteriolar constriction leads to variable glomerular perfusion
Particularly important in renal transplant recipients since FSGS can sometimes be ascribed to CNIs
Anabolic steroids used in bodybuilding
Possibly due to direct nephrotoxic effect of anabolic steroids and ↑ lean body mass
Sleep apnea
Hypoxia leads to sympathetic nervous system activation and stimulates renin-angiotensin system
Unilateral renal agenesis
Higher risk of FSGS than general population
Loss of 1 kidney later in life does not appear to cause same risk for FSGS in remaining kidney
When 1 kidney and portion of other are lost in adults, ↑ risk of FSGS development
Pathologic Consequences
Glomerular hypertrophy
↑ diameter and number of mesangial cells
Thickened GBM
Relative deficiency of podocytes, which have limited replicative ability
Segmental glomerular capillary scars and adhesions to Bowman capsule
Classically, adhesion and hyaline in perihilar region
Known as the “hilar” variant of FSGS
Animal Models
5/6 nephrectomy in rats
Widely used model
Removal/infarction of upper and lower pole of kidney followed by contralateral nephrectomy
Results in HTN, glomerulomegaly, and, later, FSGS over 8-12 weeks with proteinuria and loss of renal function
Ameliorated by inhibitors of renin-angiotensin system (angiotensin II receptor inhibitors)
Strain differences in rats and mice
CLINICAL ISSUES
Epidemiology
Incidence
Coincident with ↑ in obesity incidence: Apparent ↑ incidence of ORG
Presentation
Proteinuria
Proteinuria is often > 3.5 g/d but usually without hypoalbuminemia, hypercholesterolemia, and edema
Specifically, ORG shows lower incidence of nephrotic syndrome than idiopathic FSGS
Renal dysfunction
Most have ↑ serum creatinine and ↓ GFR preceding development of nephrotic proteinuria
ORG is notable exception since it may have ↑ GFR (supernormal, > 120 mL/min) 2° to hyperfiltration/overwork state caused by ↑ ratio of body mass to renal mass
Hypertension
ORG patients typically have a BMI > 30
BMI 30-34.9, grade 1 obesity; BMI 35.0-39.9, grade 2 obesity; and BMI ≥ 40, grade 3 obesity (morbid obesity)
Treatment
Drugs
Angiotensin II receptor antagonists
Steroids are not typically effective
Often contraindicated in many patients (e.g., in obesity) due to stimulation of weight gain and diabetes
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


