Fibromuscular Dysplasia
A. Brad Farris, III, MD
Key Facts
Terminology
Nonatherosclerotic, noninflammatory fibrous, and fibromuscular proliferation of artery, typically leading to stenosis
Clinical Issues
Mostly young and female
60-90% involve renal artery, 50% bilateral
Commonly present with hypertension
May be asymptomatic
Percutaneous transluminal renal angioplasty is treatment of choice
Image Findings
“String of beads” pattern on angiography
Microscopic Pathology
Intimal
Intimal hyperplasia resembles atherosclerosis but without lipid deposition
Medial
Medial fibroplasia with abnormally oriented smooth muscle and aneurysms is most common
Perimedial fibroplasia with fibrous band in outer media
Medial hyperplasia with hyperplastic but otherwise normal media
Periarterial (adventitial) fibroplasia
Circumferential adventitial fibrosis, normal media and intima
Top Differential Diagnoses
Atherosclerosis
Vasculitis
Dissecting aneurysm
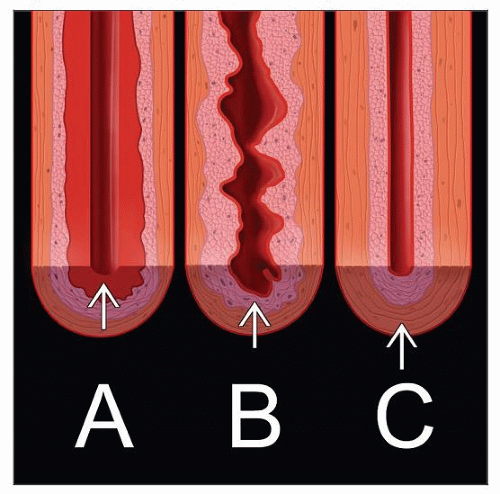 Fibromuscular dysplasia occurs in 3 main varieties: A) intimal fibroplasia, B) medial fibromuscular dysplasia, and C) periarterial (adventitial) fibroplasia. |
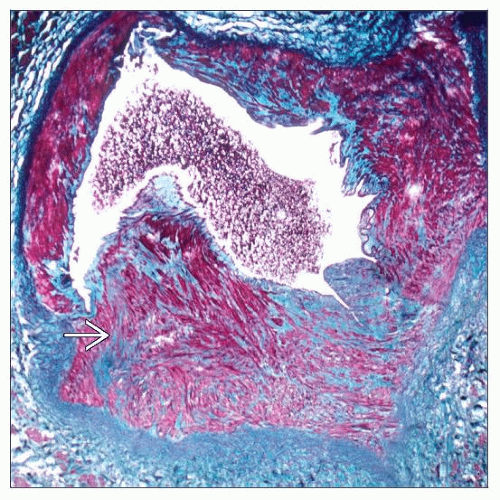 The medial fibroplasia form shows disoriented medial smooth muscle  that protrudes into the lumen of the renal artery (trichrome stain). that protrudes into the lumen of the renal artery (trichrome stain). |
TERMINOLOGY
Abbreviations
Fibromuscular dysplasia (FMD)
Synonyms
Arterial fibrodysplasia
Fibromuscular hyperplasia
Intimal or periarterial (adventitial) fibroplasia
Definitions
Idiopathic, segmental, noninflammatory, nonatherosclerotic small and medium-sized artery diseases causing stenosis and aneurysms
3 major categories
Medial
Intimal
Periarterial (adventitial)
ETIOLOGY/PATHOGENESIS
Genetic
Sibling affected in 11% of patients
Medial fibroplasia form may be congenital since it appears to be malformation
Occasionally, associated Ehlers-Danlos syndrome type IV or Marfan syndrome
1 report of increased prevalence of angiotensin converting enzyme (ACE) I allele
Environment
Smoking
Female Gender
No link to estrogens or oral contraceptives proved
CLINICAL ISSUES
Epidemiology
Incidence
Estimated 4/1,000 for symptomatic renal FMD
Medial: 60-85%
Intimal: 1-5%
Periarterial: < 1%
10-20% of patients with renal artery stenosis
Age
Younger (15-50 years) for fibromuscular dysplasia
Older (> 50 years) for fibrotic forms
Gender
Female predominance (medial form)
85% affect women under 50 years old
Male predominance (intimal form)
Site
60-90% involve renal arteries
50% bilateral
Distal 2/3 of renal artery
Extends into arcuates and interlobular arteries
May account for continued hypertension after correction of extrarenal stenosis
May have associated aneurysm
May involve multiple vascular beds
Carotid arteries (26%)
Mesenteric/intestinal arteries (9%)
Iliac arteries (5%)
Popliteal, hepatic, coronary, and subclavian arteries (9%)
Less commonly, aorta and brachial, superficial femoral, tibial, and peroneal arteries
Presentation
Hypertension
Asymptomatic
Associated with hypertrophic cardiomyopathy
Laboratory Tests
Renin levels elevated
Treatment
Surgical approaches
Surgical correction curative in ˜ 70%
Percutaneous transluminal renal angioplasty (PTRA) is treatment of choice
Complex reconstruction, such as aortorenal bypass, is required in difficult cases
Drugs
Hypertension may respond to ACE inhibitors but not most other antihypertensive agents
Prognosis
Good, if corrected
If untreated, progressive narrowing may occur over 10 years, as judged by angiography
Obstruction, dissecting aneurysms, and emboli may result
Sudden death, particularly in FMD of cardiac arteries (e.g., artery supplying the sinus node) may occur
Renal failure rare
IMAGE FINDINGS
General Features
CT and catheter angiography useful in identifying areas of stenosis or classical “string of beads” appearance
MACROSCOPIC FEATURES
General Features
Beaded pattern of aneurysms and stenosis in renal artery branches
Size
Kidney may show decreased cortical thickness
MICROSCOPIC PATHOLOGY
Histologic Features
Medial fibroplasia
Aneurysms form as a result of loss of smooth muscle and deficient elastic lamina
Fibrous and muscular ridges may be formed alternating with areas of marked thinning and even aneurysm formation
Renal infarcts are more common with this type of lesion than other types of fibromuscular dysplasia
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


