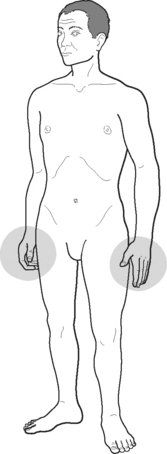
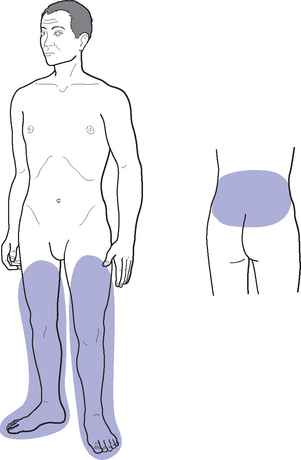
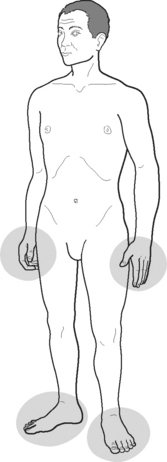
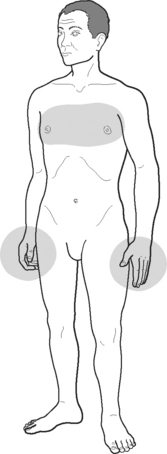
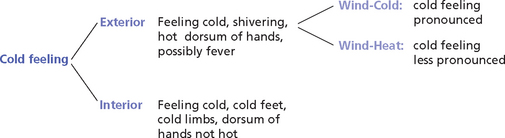
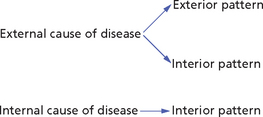
Chapter 43 Feeling of cold in interior conditions Feeling of cold in exterior conditions How to distinguish between external and internal causes of feeling of cold SIMULTANEOUS FEELING OF COLD AND FEVER IN EXTERIOR CONDITIONS ALTERNATING FEELING OF COLD AND FEELING OF HEAT FEELING OF HEAT FROM INTERNAL CAUSES CONTRADICTORY FEELINGS OF COLD AND HEAT IN INTERNAL CONDITIONS In internal conditions, questions about a patient’s feeling cold or hot are often asked towards the end of the consultation to confirm the existence of a Cold or Hot pattern. Often questions about feelings of cold or heat also help us to detect the constitutional tendency of a patient to Cold or Hot conditions. For example, patients may not have significant symptoms of Yang deficiency and Cold but, on asking, may say that they always feel cold, need to wear more clothes than other people, etc.; this symptom should never be discounted because it indicates an underlying tendency to Yang deficiency and Cold patterns. The pattern (or syndrome) refers to the location of the pathogenic factor, which may be on the Interior or Exterior: this is decided not according to the origin of the pathogenic factor but on the basis of the clinical manifestations. In other words, an external cause of disease (e.g. external Wind) may cause both an exterior pattern and an interior pattern (Fig 43.1). Fig. 43.1 Relationship between external and internal causes of disease with exterior and interior patterns Symptoms and Signs, Chapter 82 Aversion to wind means that the patient has goose pimples, dislikes going out in the wind and wants to stay indoors. Box 43.1 summarizes the clinical manifestations of Full-Cold. A deficiency of Yang of the Lungs or Heart, or both, will manifest especially with cold hands (Fig 43.2), a deficiency of Spleen-Yang with cold limbs and abdomen (Fig 43.3) and that of Kidney-Yang especially with cold legs, knees, feet and back (Fig 43.4). A deficiency of Stomach-Yang will manifest with cold epigastrium and cold limbs in a similar way to Spleen-Yang deficiency (Fig 43.3). Box 43.2 summarizes the clinical manifestations of Empty-Cold. There are however, other causes of cold limbs (as opposed to a general cold feeling). One is Qi stagnation: when Qi stagnates it may fail to reach the hands and feet and these become cold (Fig 43.5). This is called the ‘Four Rebellious Syndrome’, in which the ‘Four Rebellious’ indicate cold hands and feet; the famous formula Si Ni San Four Rebellious Powder is used for this pattern. An important difference between cold in the limbs due to Yang deficiency and that due to Qi stagnation is that in the former case the whole limb will be cold whereas in the latter case only the hands and feet, and especially the fingers, are cold. Besides this, cold limbs may also derive in women from Blood deficiency; this is due to the deficient Blood not reaching the extremities. In cases of Heart-Blood deficiency only the hands and chest will be cold (Fig 43.6), whereas in cases of Liver-Blood deficiency the feet will be cold (Fig 43.7). Box 43.3 summarizes the patterns underlying a cold feeling and cold limbs in interior conditions. The areas that are usually touched to gauge this are the dorsum of the hands and the forehead. It should be stressed that the feeling of cold and fever (or body feeling hot to the touch) are simultaneous and not alternating: thus, if a patient feels cold in the morning without a fever and without body feeling hot to the touch and has a fever in the evening, this would correspond to the Lesser-Yang syndrome and would not constitute the beginning stage of an invasion of Wind. Figure 43.8 differentiates the manifestations of cold feeling in exterior and interior conditions. Box 43.4 summarizes the clinical manifestations of interior and exterior pathogenic factors. When the patient suffers from interior Cold, there are none of the above symptoms. Another distinction between a cold feeling in exterior syndromes and one in interior syndromes is that in the former case the cold feeling is not alleviated by covering oneself, while in the latter case it is. In fact patients who feel cold and shiver from an invasion of exterior Wind will want to go to bed and cover up with blankets, but this will not alleviate the cold feeling and shivering. If a patient suffers from internal Cold, this will be alleviated by covering oneself. Table 43.1 summarizes the differentiation between external and internal Cold. Table 43.1 Differentiation between external and internal Cold A simultaneous feeling of cold and fever indicates the invasion of an exterior pathogenic factor and that this factor is still on the Exterior. The simultaneous presence of a cold feeling or shivers with a fever, or both, usually indicates an acute invasion of Wind and it denotes that the pathogenic factor is still on the Exterior: as long as there is a feeling of cold the pathogenic factor is on the Exterior. The clinical situations when the pathogenic factor is on the Exterior are described in the Greater-Yang pattern within the Six Stages from the ‘Discussion of Cold-induced Diseases’ (Shang Han Lun) and the Defensive-Qi level within the Four Levels described by the School of Warm Diseases (Wen Bing) of the Qing dynasty (see Part 6). As mentioned above, it is important to stress that the feeling of cold and fever (or body feeling hot to the touch) are simultaneous and not alternating (Fig 43.9).
 FEELING OF COLD, FEELING OF HEAT AND FEVER
FEELING OF COLD, FEELING OF HEAT AND FEVER
WHEN WE ASK
HOW WE ASK
Terminology
FEELING OF COLD
Feeling of cold in interior conditions
Feeling of cold in exterior conditions
External invasions
How to distinguish between external and internal causes of feeling of cold
External invasion of Cold
Internal Cold
Feels cold, shivers, dislikes going out, fever, sneezing, cough, sore throat, nasal discharge
Feels cold, none of the symptoms associated with an external invasion is present
Cold feeling not alleviated by wrapping up in clothes and blankets
Cold feeling is alleviated by wrapping up warm
SIMULTANEOUS FEELING OF COLD AND FEVER IN EXTERIOR CONDITIONS
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Basicmedical Key
Fastest Basicmedical Insight Engine