CHAPTER 26 External skull
The skull is the bony skeleton of the head. It shields the brain, the organs of special sense and the cranial parts of the respiratory and digestive systems, and provides attachments for many of the muscles of the head and neck. Movement of the lower jaw (mandible) occurs at the temporomandibular joint.
FRONTAL (ANTERIOR) VIEW
Viewed from the front, the skull is generally ovoid in shape and is wider above than below (Fig. 26.1). The upper part is formed by the frontal bone which underlies the forehead region above the orbits. Superomedial to each orbit is a rounded superciliary arch (more pronounced in males) between which there may be a median elevation, the glabella. The glabella may show the remains of the inter-frontal (metopic) suture, which is present in about 9% of adult skulls. Above each superciliary arch is a slightly elevated frontal tuber or eminence which is generally more obvious in the female. Below, where the nasal bones meet the frontal bone, is a depression marking the root of the nose. The frontal bone articulates with the two nasal bones at the frontonasal sutures; the point at which the frontonasal and internasal sutures meet is the anthropometric landmark known as the nasion.
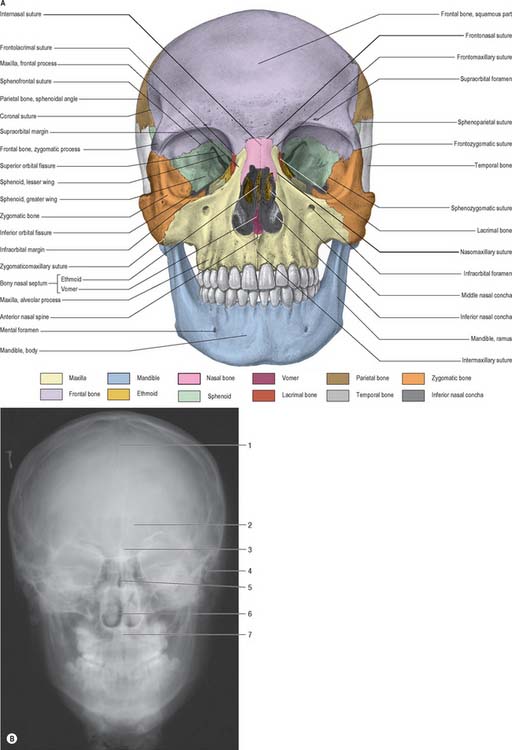
A (From Sobotta 2006.) (B by courtesy of Mr Eric Whaites, Dental Institute, King’s College, London.)
The upper part of the face is occupied by the orbits and the bridge of the nose. Each orbital opening is approximately quadrangular (see Ch. 39). The upper, supraorbital, margin is formed entirely by the frontal bone, interrupted at the junction of its sharp lateral two-thirds and rounded medial third by the supraorbital notch or foramen, which transmits the supraorbital vessels and nerve. The lateral margin of the orbit is formed largely by the frontal process of the zygomatic bone and is completed above by the zygomatic process of the frontal bone; the suture between them lies in a palpable depression. The infraorbital margin is formed by the zygomatic bone laterally and maxilla medially. Both lateral and infraorbital margins are sharp and palpable. The medial margin of the orbit is formed above by the frontal bone and below by the lacrimal crest of the frontal process of the maxilla.
The anterior nasal aperture is piriform in shape, and is wider below than above and bounded by the nasal bones and maxillae. The upper boundary of the aperture is formed by the nasal bones while the remainder is formed by the maxillae. In life, various cartilages (septal, lateral nasal, major and minor alar) help to delineate two nasal cavities (see Ch. 32). The defleshed skull presents a single anterior nasal aperture because these cartilages are lost during preparation or decomposition. However, the shape of these bones can be used quite successfully to predict the shape of the cartilaginous nose.
AP radiographs of the skull clearly show the central location of the paranasal air sinuses in the frontal bone, the maxilla and the ethmoid. These can be particularly useful indicators of identity when postmortem images are compared with premortem clinical films.
POSTERIOR VIEW
The parietal, temporal and occipital bones form the entirety of the posterior view (Fig. 26.2). The superolateral region is occupied by the parietal bones, the mastoid part of the temporal bones comprises the inferolateral regions and the central portion is occupied by the occipital bone, which is why this aspect is also referred to as the occipital view. The parietal bones articulate with the occipital bone at the lambdoid suture and extend inferiorly into the occipitomastoid and the parietomastoid sutures behind and above the mastoid process respectively. Sutural or wormian bones are islands of bone that are commonly found within the lambdoid suture. They may arise from separate centres of ossification and they appear to have no clinical significance, being of genetic rather than pathological aetiology. A large interparietal bone is not uncommon and is sometimes referred to as an Inca bone (Fig. 26.2).
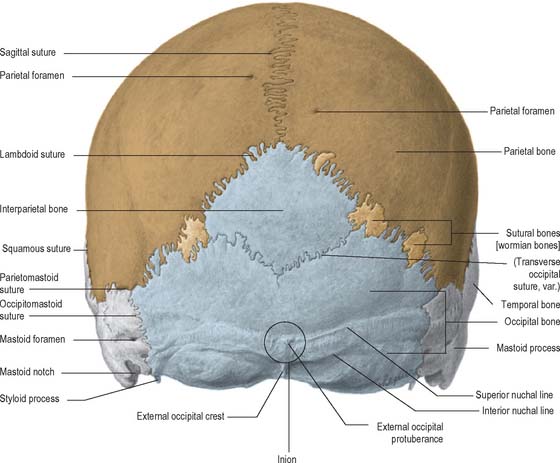
The external occipital protuberance is a midline ridge or a distinct process on the occipital bone which can become particularly well developed in the male. Superior nuchal lines extend laterally from the protuberance and represent the boundary between the scalp and the neck. Inferior nuchal lines run parallel to, and below, the superior nuchal lines; a set of highest nuchal lines may sometimes occur above the superior lines. The external occipital protuberance, nuchal lines and roughened external surface of the occipital bone between the nuchal lines, all afford attachment to muscles of the neck.
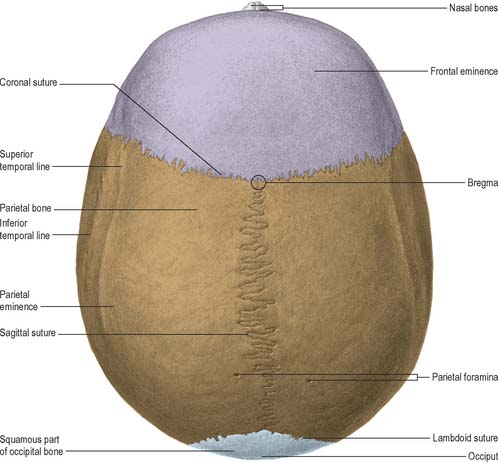
SUPERIOR VIEW
Seen from above, the contour of the cranial vault varies greatly but is usually ellipsoid, or more strictly, a modified ovoid with its greatest width lying nearer to the occipital pole (Fig. 26.3). Four bones constitute this view and articulate via three well-defined sutures. The squamous part of the frontal bone is anterior, the squamous part of the occipital bone is posterior and the two parietal bones meet in the midline and separate the frontal from the occipital bone. The maximal parietal convexity on each site is palpable at the parietal tuber or eminence: it is most conspicuous in the female who ostensibly retains a paedomorphic appearance. The superior and inferior temporal lines run close to the parietal eminence but are best seen in a lateral view.
LATERAL VIEW
The skull, viewed from the side, can be subdivided into three zones: face (anterior); temporal region (middle); occipital region (posterior) (Fig. 26.4). The face has been considered in the section on the anterior view of the skull.
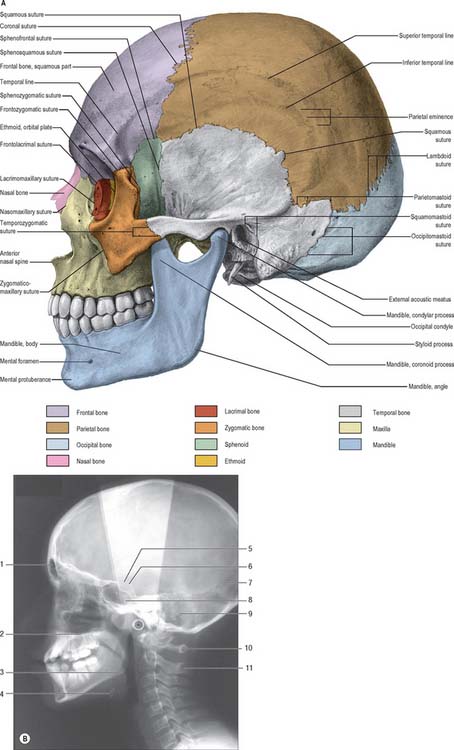
A (From Sobotta 2006.) (B by courtesy of Mr Eric Whaites, Dental Institute, King’s College, London.)
The lateral surface of the ramus of the mandible will be described briefly here as its position lies within the middle region of this view of the skull (see Ch. 31). The ramus is a plate of bone projecting upwards from the back of the body of the mandible; its lateral surface gives attachment to masseter. The ramus bears two prominent processes superiorly, the coronoid process anteriorly and condylar process posteriorly, separated by the mandibular notch. The coronoid process is the site of insertion of temporalis and the condylar process articulates with the mandibular fossa of the temporal bone at the temporomandibular joint. The inferior and posterior borders of the mandible meet at the angle, which is often splayed in the male because of the larger site of muscle attachment for medial pterygoid on the internal surface.
The mandibular (glenoid) fossa is the part of the temporomandibular joint with which the condylar process of the mandible articulates. It is bounded in front by the articular eminence and behind by the tympanic plate. The articular eminence provides a surface over which the mandibular condyle glides during mandibular movements (see Ch. 31).
The tympanic plate of the temporal bone contributes most of the margin of the external acoustic (auditory) meatus, and the squamous part forms the posterosuperior region (see Ch. 36). The external margin is roughened to provide an attachment for the cartilaginous part of the meatus. A small depression, the suprameatal triangle, lies above and behind the meatus and is related to the lateral wall of the mastoid antrum.
The infratemporal fossa is an irregular postmaxillary space located deep to the ramus of the mandible; it communicates with the temporal fossa deep to the zygomatic arch (see Ch. 31). It is best visualized, therefore, when the mandible is removed but, for completeness, is considered here. Its roof is the infratemporal surface of the greater wing of the sphenoid. The lateral pterygoid plate lies medial to the fossa and the ramus of the mandible and styloid process lie laterally and posteriorly respectively. The infratemporal fossa has no anatomical floor. Its anterior and medial walls are separated above by the pterygomaxillary fissure lying between the lateral pterygoid plate and the posterior wall of the maxilla. The infratemporal fossa communicates with the pterygopalatine fossa through the pterygomaxillary fissure.
INFERIOR (BASAL) VIEW
The inferior surface of the skull, the base of the cranium, is complex: it extends from the upper incisor teeth anteriorly to the superior nuchal lines of the occipital bone posteriorly (Fig. 26.5). The region contains many of the foramina through which structures enter and exit the cranial cavity. The inferior surface can be conveniently subdivided into anterior, middle, posterior and lateral parts. The anterior part contains the hard palate and the dentition of the upper jaw and lies at a lower level than the rest of the cranial base. The middle and posterior parts can be arbitrarily divided by a transverse plane passing through the anterior margin of the foramen magnum. The middle part is occupied mainly by the base of the sphenoid bone, the apices of the petrous processes of the temporal bones and the basilar part of the occipital bone. The lateral part contains the zygomatic arches, mandibular fossa, tympanic plate and the styloid and mastoid processes. The posterior part lies in the midline and is exclusively formed from the occipital bone. Whereas the middle and posterior parts are directly related to the cranial cavity (the middle and posterior cranial fossae), the anterior part (the palate) is some distance from the anterior cranial fossa, being separated from it by the nasal cavities.
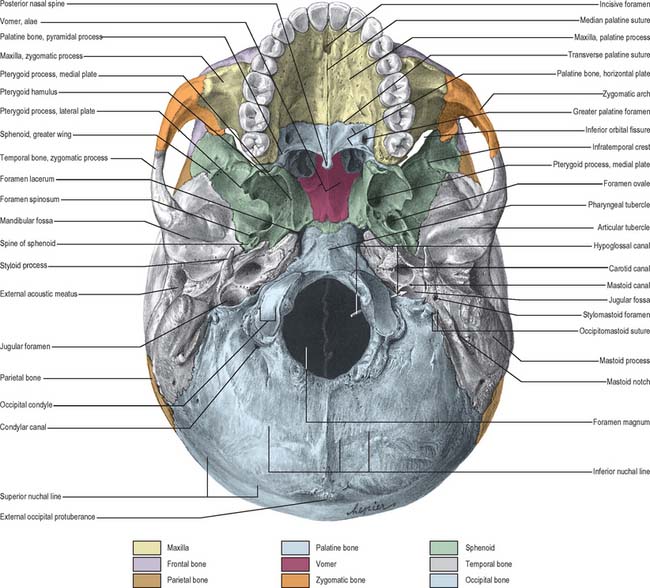
ANTERIOR PART OF CRANIAL BASE
The bony palate within the superior alveolar arch is formed by the palatine processes of the maxillae anteriorly and the horizontal plates of the palatine bones posteriorly, all meeting at a cruciform system of sutures (Fig. 26.5). The median palatine suture runs anteroposteriorly and divides the palate into right and left halves. This suture is continuous with the intermaxillary suture between the maxillary central incisor teeth. The transverse palatine (palatomaxillary) sutures run transversely across the palate between the maxillae and the palatine bones. The palate is arched sagittally and transversely: its depth and breadth are variable but are always greatest in the molar region. The incisive fossa lies behind the central incisor teeth, and the lateral incisive foramina, through which incisive canals pass to the nasal cavity, lie in its lateral walls. Median incisive foramina are present in some skulls and open onto the anterior and posterior walls of the fossa. The incisive fossa transmits the nasopalatine nerve and the termination of the greater palatine vessels. When median incisive foramina occur, the left nasopalatine nerve usually traverses the anterior foramen and the right nerve traverses the posterior foramen. The greater palatine foramen lies near the lateral palatal border of the transverse palatine suture; a vascular groove, deeper behind and shallower in front, leads forwards from the foramen. The lesser palatine foramina, usually two, lie behind the greater palatine foramen and pierce the pyramidal process of the palatine bone which is wedged between the lower ends of the medial and lateral pterygoid plates. The palate is pierced by many other small foramina and is marked by pits for palatine glands. Variably prominent palatine crests extend medially from behind the greater palatine foramina. The posterior border projects back as the posterior nasal spine. In the adult, the alveolar arch bears a maximum of 16 sockets or alveoli for the teeth: the sockets vary in size and depth, some are single and some are subdivided by septa, according to the morphology of the dental roots.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


