Patient Story
A 12-year-old Hispanic girl, accompanied by her mother, presents with a 1-year history of a red irritated rash in both axillae (Figure 119-1). She has been seen by multiple physicians and many antifungal creams had been tried with no results. Even hydrocortisone did not help. She had stopped wearing deodorant for fear that she was allergic to all deodorants. Although the rash barely fluoresced at all, the physical examination and history were most consistent with erythrasma. The patient was given a prescription for oral erythromycin and the erythrasma cleared to the great delight of the patient and her mother.

Introduction
Epidemiology
- The incidence of erythrasma is approximately 4%.1
- Both sexes are equally affected.
- The inguinal location is more common in men.
Etiology and Pathophysiology
- Corynebacterium minutissimum, a lipophilic Gram-positive non-spore-forming rod-shaped organism, is the causative agent.
- Under favorable conditions, such as heat and humidity, this organism invades and proliferates the upper one-third of the stratum corneum.
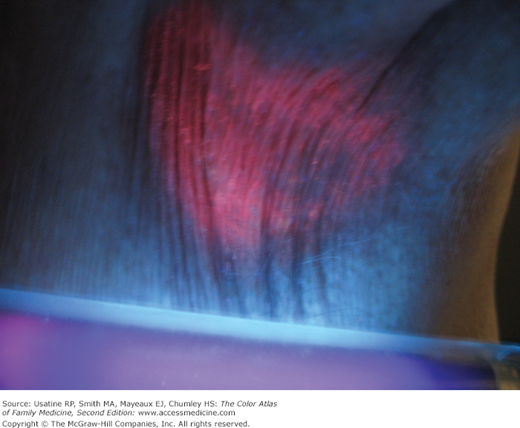
- The organism produces porphyrins that result in the coral red fluorescence seen under a Wood lamp (Figure 119-2).
Risk Factors
Diagnosis
- Erythrasma is a sharply delineated, dry, red-brown patch with slightly scaling patches. Some lesions appear redder, whereas others have a browner color (Figures 119-3 and 119-4).
- The lesions may appear with central clearing and be slightly raised from the surrounding skin (Figure 119-5).
- The lesions are typically asymptomatic; however, patients sometimes complain of itching and burning when lesions occur in the groin (Figure 119-6).





