TERMS
•Percentage of error
•Sensitivity requirement
•Tablespoon
•Teaspoon
OBJECTIVES
Upon completion of this chapter, the technician student will be able to:
•Recognize and describe equipment used to measure volume and weight.
•Determine the best instrument for measuring large amounts and single-dose quantities.
•Define and calculate percentage of error for volume and weight measurements.
•Calculate the smallest amount to be measured by a given device.
This chapter introduces the pharmacy technician student to equipment and methods used to measure volume and weight. It also discusses equipment used for measuring large and small single-dose volumes and weights and percentage of error. The increasing number of compounding pharmacies and the increasing number of compounded prescriptions means that the pharmacy technician in today’s practice must be able to use calculations introduced in this chapter.
 Measurement of Volume
Measurement of Volume
Common instruments for the pharmaceutical measurement of volume range from micropipets and burettes used in analytical procedures to large, industrial-size calibrated vessels. The selection of measuring instrument should be based on the level of precision required. In pharmacy practice, the most common instruments for measuring volume are cylindric and conical (cone-shaped) graduates, as shown in Figures 4.1 and 4.2. For the measurement of small volumes, however, the pharmacist often uses a calibrated syringe or a pipet.

Figure 4.1Cylindrical graduates.

Figure 4.2Conical graduates.
Whereas cylindrical graduates are calibrated in metric units, conical graduates are usually dual scale, that is, calibrated in both metric and apothecary units of volume. Metric units of volume and apothecaries’ units are described in Chapter 2. Both glass and plastic graduates are commercially available in a number of capacities, ranging from 5 to 1000 mL and greater.
Graduate Selection Rule

It is best to select the graduate with a capacity equal to or just exceeding the volume to be measured.
Measurement of small volumes in large graduates tends to increase the size of the error. The design of a volumetric apparatus is an important factor in measurement accuracy; the narrower the bore or chamber, the less the error in reading the meniscus and the more accurate the measurement (Fig. 4.3).
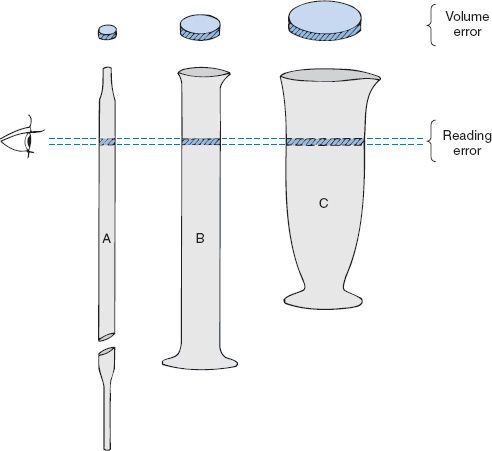
Figure 4.3Volume error differentials due to instrument diameters.
According to the United States Pharmacopeia, a deviation of ±1 mm in the meniscus reading causes an error of approximately 0.5 mL when a 100-mL cylindrical graduate is used and an error of 1.8 mL at the 100-mL mark in a comparable conical graduate.1 In conformity with the legal requirements for pharmaceutical graduates, as stated in the National Bureau of Standards Handbook 44, a graduate shall have an initial interval that is not subdivided, equal to not less than one-fifth and not more than one-fourth of the capacity of the graduate.2 Conical graduates of less than 25-mL capacities are not recommended for use in pharmaceutical compounding.
It is essential for the pharmacy technician to select the proper type and capacity of instrument for volumetric measure and to carefully observe the meniscus at eye level to achieve the desired measurement.
It is equally important to have the proper equipment for measuring doses. According to the United Stated Pharmacopoeia, “For household purposes, an American Standard Teaspoon has been established by the American National Standards Institutes as containing 4.92 ± 0.24 mL.” In view of the almost universal practice of using teaspoons ordinarily available in the household for the administration of medicine, the teaspoons may be regarded as representing 5 mL. Preparations intended for administration by teaspoon should be formulated on the basis of dosage in 5-mL units. Any dropper, syringe, medicine cup, special spoon, or other device used to administer liquids should deliver 5 mL whenever a teaspoon calibration is indicated.
teaspoon The household unit of measure that is equivalent to 5 mL.
For liquid medications, it is recommended that patients be directed to use a pharmaceutically calculated dose spoon or medicine cup to ensure the greatest accuracy possible.
Through habit and tradition the fluidram is used by some physicians in the signa portion of the prescription when indicating teaspoonful dosage. The technician may interpret this symbol as a teaspoonful in dispensing prefabricated manufacturers’ products called for on prescriptions and allow the patient to use the household teaspoon. Doses less than a teaspoonful (usually for children) are often indicated on the label as fractions of a teaspoonful, such as ¼ or ½ tsp. Sometimes doses are not readily converted to a fraction of a teaspoonful, and then the patient must be directed to take the correct number of milliliters. In these cases it is advisable to provide the patient with a medication spoon with milliliters marked or an oral syringe. An oral syringe (Fig. 4.4) is the best device for measurements that do not translate into a fractional part of a teaspoon. Oral syringes are used to deliver oral liquids to infants and small children. Oral syringes are calibrated in metric units and household units and come in a variety of sizes to ensure accuracy in dosing small amounts. An oral syringe should never be confused with a syringe used for injections. Serious medication errors may result from using a syringe for a purpose other than the intended one. A medicine cup (Fig. 4.5) is the best choice for large dose amounts, such as 2 tsp to 2 tbs. It is important to advise the patients or caregivers on the proper measuring devices and to provide them with the appropriate device. The technician should make sure that the language on the label matches that of the oral syringe or medication spoon. For example, do not label the product in cubic centimeters if the oral syringe has markings in milliliters.
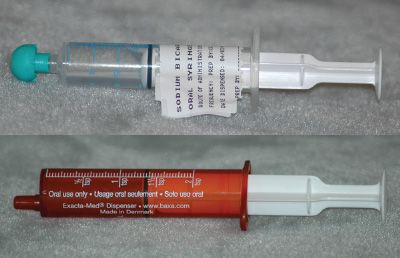
Figure 4.4 Two oral syringes, one clear and one amber colored to protect the medication from light. The amber-colored oral syringe is calibrated in 0.2-mL increments and marked in 1/2-tsp increments up to 2 tsp.

Figure 4.5A medicine cup.
For the patient, liquid dosage is usually measured in household terms, most commonly by the teaspoonful or tablespoonful. Orders are often written in metric measures or common measures; for example, 5 mL or 1 fl oz (Table 4.1). In calculating doses, pharmacists and physicians accept a capacity of 5 mL for the teaspoonful and 15 mL for the tablespoonful. The capacities of household teaspoons vary from 3 to 7 mL, and those of tablespoons vary from 15 to 22 mL. Such factors as viscosity and surface tension of a given liquid and the technique of the person measuring the liquid can influence the actual volume held by a household spoon.
tablespoon The household unit of measure that is equivalent to 15 mL.
Critical Thinking 4.1




