Epilepsies with Onset during Infancy (2 to 12 Months)
Epilepsies with Onset during Infancy (2 to 12 Months)
The epilepsies and epilepsy syndromes with onset during infancy (2 to 12 months) and accompanying seizure types are listed in Table 5-1.
I. SYMPTOMATIC AND PROBABLY SYMPTOMATIC FOCAL EPILEPSIES
Focal/symptomatic epilepsies can occur at any age. Three seizure types occur with these epilepsies: simple partial (focal); complex partial (psychomotor, temporal lobe); and tonic-clonic (grand mal). The clinical and electroencephalographic (EEG) features of these three seizure types are reviewed in Chapter 2. Differential diagnostic entities to consider in children and adults when diagnosing these seizure types are listed in Chapter 2 and reviewed in Chapter 9.
Depending on locus of onset, five symptomatic and probably symptomatic epilepsy syndromes have been recognized (Table 5-1). Clinical and EEG features, management, and prognosis of these syndromes are reviewed in Chapter 3.
One special symptomatic focal epilepsy deserves special consideration. The hemiconvulsion-hemiplegia syndrome (HHS) is a rare form of symptomatic epilepsy that usually begins during the first 2 years of life. A sudden and prolonged unilateral clonic seizure is followed by unilateral hemiparesis. The event occurs suddenly in an otherwise healthy child. In 80% of patients, unilateral seizures later develop to complete the hemiconvulsion-hemiplegia epilepsy syndrome (HHES). Perhaps because of better treatment of status epilepticus, the condition is now rare.
II. GENERALIZED/SYMPTOMATIC EPILEPSIES
Four generalized/symptomatic epilepsies (West syndrome, tonic seizures, atonic seizures, and Lennox-Gastaut syndrome) are true age-dependent epileptic conditions. West syndrome and Lennox-Gastaut syndrome always begin during early childhood, and the vast majority of patients with tonic and atonic seizures have seizure onset during the first year of life.
These conditions are classified as generalized seizures because the clinical and EEG features typically suggest widespread involvement of the cortex. However, in many of these patients, the seizures have a partial onset with rapid secondary generalization.
A. West Syndrome (Infantile Spasms)
Clinical and EEG features of seizures in children vary as a function of age. A good example of these age-related phenomena is infantile spasms, a unique seizure disorder confined to early childhood; infantile spasms are an age-specific disorder occurring in children only during the first 2 years of life. The peak age at onset is between 4 and 6 months, and approximately 90% of infantile spasms begin before 12 months of age. The incidence of infantile spasms is estimated at 0.4 in 1,000 live births.
Table 5-1. Groups of specific epilepsy syndromes and specific epilepsy syndromes with onset during infancy (2-12 months) and accompanying seizure types
Symptomatic and probably symptomatic focal epilepsies
The characteristic features of this syndrome are myoclonic seizures, hypsarrhythmic EEG, and mental retardation. This triad is sometimes referred to as West syndrome. As will be seen, however, not all cases conform strictly to this definition. The disorder is also referred to in the literature as massive spasms, salaam seizures, flexion spasms, jackknife seizures, massive myoclonic jerks, and infantile myoclonic seizures.
2. Seizure Phenomena
Infantile spasms may vary considerably in their clinical manifestations. Some seizures are characterized by brief head nods; other seizures consist of violent flexion of the trunk, arms, and legs. The diagnosis may often be delayed because the parents and even the family physician may not recognize spasms as seizures. What usually does not vary is that in each child, the spasms are stereotyped. In addition, spasms characteristically occur in flurries.
Although it resembles a myoclonic or tonic seizure, the spasm is a distinct type of seizure. A myoclonic jerk is a rapid, shocklike contraction of limited duration, whereas the tonic seizure is a prolonged muscle contraction of growing intensity. The true spasm consists of a characteristic muscular contraction that lasts from 1 to 2 seconds and reaches a peak more slowly than a myoclonic jerk, but more rapidly than a tonic seizure.
The seizures in infantile spasms are of three types: flexor, extensor, and mixed flexor-extensor. Flexor spasms consist of brief contractions of flexor musculature of the neck, trunk, arms, and legs. Spasms of the muscles of the upper limbs result either in adduction of the arms in a self-hugging motion or in abduction of the arms to either side of the head with the arms flexed at the elbow. Extensor spasms consist predominantly of extensor muscle contractions, producing abrupt extension of the neck and trunk with extensor abduction or adduction of the arms, legs, or both. Mixed flexor-extensor spasms include flexion of the neck, trunk, and arms and extension of the legs, or flexion of the legs and extension of the arms with varying degrees of flexion of the neck and trunk. Asymmetric spasms occasionally occur and resemble a fencing posture. Infantile spasms are frequently associated with eye deviation or nystagmus.
Asymmetric spasms can be seen when the muscular contractions do not occur simultaneously on the two sides of the body. This type of spasm is usually observed in symptomatic infants with severe brain lesions, agenesis of the corpus callosum, or both. Focal signs, such as eye or head deviation, may accompany symmetric and asymmetric spasms. Asymmetric spasms generally are isolated, but they can also follow or precede a partial seizure, or sometimes appear simultaneously with a partial or generalized seizure.
Infantile spasms frequently occur in clusters, and the intensity and frequency of the spasms in each cluster may increase to a peak before progressively decreasing. The number of spasms per cluster varies considerably, with some clusters having more than 30 spasms. The number of clusters per day also varies, with some patients having more than 20 clusters per day. Clusters can occur at night, although they rarely occur during sleep. Crying or irritability during or after a flurry of spasms is commonly observed.
3. Electroencephalographic Phenomena
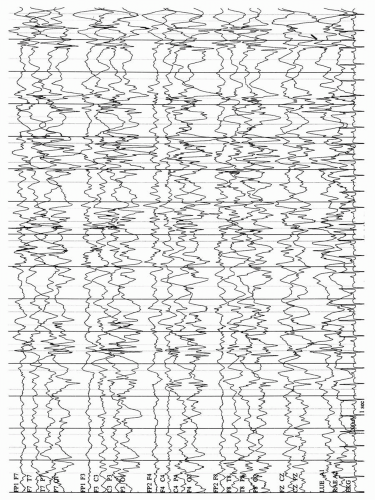
Infantile spasms are associated with markedly abnormal EEGs. The most commonly seen interictal pattern is hypsarrhythmia, which consists of very high-voltage, random, slow waves and multifocal spikes and sharp waves (Fig. 5-1). The chaotic appearance of the EEG abnormality gives the impression of total disorganization of cortical voltage and rhythms. During sleep, bursts of polyspike and slow waves occur. Somewhat surprising, in view of the marked background abnormalities, is the persistence of sleep spindles in some patients. During rapid eye movement (REM) sleep, a marked diminution or complete disappearance of the hypsarrhythmic pattern may diminish markedly or disappear. Infantile spasms are associated with a decrease of the total sleep time, as well as a decrease in REM sleep. Variations in hypsarrhythmia have been described, including patterns with interhemispheric synchrony, a consistent focus of abnormal discharge, episodes of attenuation, and high-voltage slow activity with few sharp waves or spikes. The variant patterns of hypsarrhythmia are frequent and do not correlate with prognosis.
Although a hypsarrhythmic or modified hypsarrhythmic pattern is the most common type of interictal abnormality seen in infantile spasms, this EEG pattern may not be present in some patients with infantile spasms. Some patients with infantile spasms do not have hypsarrhythmia early in the course of the disorder, but the pattern develops later. Although hypsarrhythmia is primarily associated with infantile spasms, it occurs in other disorders as well.
Fig. 5-1. Hypsarrhythmia in an infant with infantile spasms. Note high-amplitude, disorganized background with multifocal spikes and sharp waves. EKG, electrocardiogram.
Like the interictal pattern, the ictal EEG changes during infantile spasms are variable. The most characteristic ictal EEG pattern of the spasms consists of a positive wave over the vertexcentral region; low-amplitude fast (14 to 16 Hz) activity, or a diffuse flattening, called decremental activity, may also be seen.
The presence of focal features is one of the variations of the basic hypsarrhythmic patterns and may be associated with partial seizures. Partial seizures may precede, accompany, or follow the cluster of spasms. This observation suggests that cortical “pacemakers” may be important in the development of infantile spasms.
EEGs are not static in this disorder and may evolve over time. Some patients with spasms may not have hypsarrhythmia at the onset of their disorder. Other patients may have slow EEG recordings with rare epileptiform activity that then develops into hypsarrhythmic patterns. Follow-up EEG recordings may be necessary to demonstrate hypsarrhythmia.
4. Basic Mechanisms
The clinical and ictal EEG features of infantile spasms are suggestive of a generalized seizure disorder, yet some children with infantile spasms respond to surgical removal of a cortical lesion. For that reason, the brainstem, which has widespread projections throughout the central nervous system, has been implicated as playing an important role in the genesis of infantile spasms. An underlying disruption of neuronal function within specific nuclei of the pontine reticular formation could result in interference with descending pathways that exert control over spinal reflexes and result in infantile spasms. In addition, the hypsarrhythmic EEG pattern could be the result of abnormal input to the thalamic and cortical neurons through ascending projections.
5. Differential Diagnosis
Because infantile spasms differ significantly from the clinical features of other seizures in young children, it is not surprising that parents and primary caregivers may miss the diagnosis. Yet the pediatrician or family physician rarely has the opportunity actually to see the spasms and must depend on the description by the parents. With increasing use of home videotaping and greater awareness of the problem, the delay in diagnosis is being reduced. Occasionally, the clinical course is atypical, and the spasms do not occur in clusters, or involve only slight movements or episodes of akinesia. In these patients, the EEG is helpful, because it is invariably abnormal.
A few other conditions may be confused with infantile spasms. Early myoclonic epileptic encephalopathy (EMEE) and early infantile epileptic encephalopathy (EIEE) have a clinical similarity to infantile spasms. EMEE is characterized clinically by the occurrence of sporadic and erratic fragmentary myoclonus, usually in association with other seizure types. The seizures usually begin in the neonatal period. The EEG demonstrates burst-suppression. A variety of etiologic agents have been associated with the disorder, including metabolic diseases, cerebral dysgenesis, and hypoxic-ischemic insults. The prognosis in the disorder is severe; most infants die within 1 year or have severe neurologic sequelae.
EIEE, also termed Ohtahara syndrome, is reviewed in Chapter 4.
Benign nonepileptic infantile spasms is a syndrome that begins in infancy with flexion spasms. However, the syndrome differs from West syndrome by the absence of mental retardation or regression and the presence of normal EEGs during both wakefulness and sleep.
Benign neonatal sleep myoclonus, which was discussed with neonatal seizures, in Chapter 4, section I.D, may be confused with infantile spasms. The EEG is very helpful in distinguishing the two conditions.
6. Etiology
On the basis of history, physical examination, and laboratory studies, cases of infantile spasms have been conventionally classified into those in which no preceding neurologic disorder or identified etiologic factor (idiopathic) is apparent, and those in which a preexisting, presumptively responsible pathologic event or disorder is demonstrated (symptomatic cases). Some authors use another category, cryptogenic, to refer to children who have developmental delay or an abnormal neurologic examination before the onset of spasms, but in whom an etiology cannot be sufficiently identified.
As can be seen in Table 5-2, infantile spasms have been associated with a wide variety of etiologies. Virtually any disorder that can cause brain damage can be associated with infantile spasms. Infantile spasms are particularly prevalent among children with tuberous sclerosis complex, and tuberous sclerosis complex (TSC) accounts for up to 25% of infantile spasms cases. TSC is a congenital syndrome characterized by the widespread development of benign tumors in multiple organs, somewhat different that those seen in classic West syndrome. In TSC, focal seizures can precede, coexist with, or evolve into infantile spasms. EEG features of focal or multifocal spikes are most common when seizures are first identified, with hypsarrhythmia (often with focal features) evolving later.
Only gold members can continue reading. Log In or Register to continue