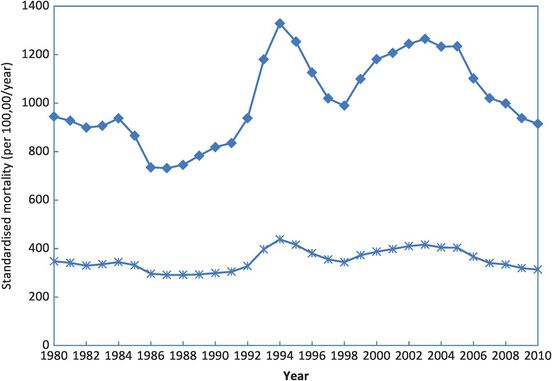
Time trends in lung cancer mortality rates in the USA (age-standardised to the 1970 US population) for white men (––) and women (___).
The derivation of the word ‘epidemiology’ itself is from the Greek epi, upon, demos, the people, and logia, study. Literally, therefore, it means the ‘study (of what is) upon the people’. Such study suggests a simple set of questions that have long lain at the heart of epidemiology.
What disease/condition is present in excess?
Who is ill?
Where do they live?
When did they become ill?
Why did they become ill?
The first question reflects the need for a sound, common definition of a disease so that like is compared with like. Epidemiology is all about comparison – without some reference to what is usual, how can we identify excess? The next three questions form the mantra of descriptive epidemiology: ‘person, place and time’. As Figure 1.2 shows, an ‘epidemic of premature mortality’ occurred among young and middle-aged men in Russia in the mid-1990s and again in the early 2000s. This description captures the essence of the problem and prompts the next questions: what caused these epidemics? What changed in the circumstances of younger Russian men to reverse the pattern of falling mortality in the early 1980s and then cause it to almost double in less than 10 years? And why did this happen again in the late 1990s? Other data show that there were no such mortality changes in Western Europe, or among older Russian men or infants, or (to the same extent) in Russian women. This simple graph captures a public health disaster for Russia and prompts urgent causal speculation: Why did this happen? Solving and responding to this final question is critical for public health progress, but there is clearly no simple solution. In this case, a high proportion of the deaths were linked to excess consumption of alcohol during the 1990s: increases in mortality coincided with periods of economic and societal crisis, and rates fell when the economic situation improved (Zaridze et al., 2009). The earlier decline during the 1980s coincided with an anti-alcohol campaign involving higher taxes and reduced production which led to sharp decreases in alcohol consumption in the short term, and lower rates of alcohol-related mortality and suicide (Pridemore and Spivak, 2003). This example highlights the importance of paying close attention to descriptive data that provide a ‘community diagnosis’ or take the public health ‘pulse’ of a nation. Much can be gleaned from apparently simple data to give a quite precise description of the overall health of a population or a more specific health event, as the following exercise shows.
Changes in all cause mortality at ages 0–64 years in the Russian Federation from 1980 to 2010 (◆men,  women).
women).
An historical epidemic
Table 1.3 shows some data that relate to an actual human experience. It tells you how many people there were in various age, sex and socioeconomic groups and what percentage of these people died during the ‘epidemic’. The challenge is to use these data to describe the event systematically in terms of whom this happened to (we have no data on place or time) and then to think about the sort of event that might have induced such a pattern.
| SESa | Adult males | Adult females | Children (both sexes) | Total population | ||||
|---|---|---|---|---|---|---|---|---|
| Total | % Dead | Total | % Dead | Total | % Dead | Total | % Dead | |
| High | 175 | 67.4 | 144 | 2.8 | 6 | – | 325 | 37.5 |
| Medium | 168 | 91.7 | 93 | 14.0 | 24 | – | 285 | 58.6 |
| Low | 462 | 83.8 | 165 | 53.9 | 79 | 65.8 | 706 | 74.8 |
| Other | 885 | 78.3 | 23 | 13.0 | 0 | – | 908 | 76.7 |
| Total | 1690 | 80.0 | 425 | 25.6 | 109 | 47.7 | 2224 | 68.0 |
a SES, socioeconomic status.
The following questions are designed to help you identify key features of the data.
1. What is distinctive about this isolated population with regard to:
the numbers of men and women (sex distribution),
the numbers of adults and children (age distribution), and
the numbers in each socioeconomic group (socioeconomic distribution)?
2. What strikes you about the percentage of people who died (the ‘death rate’)? Is this different for (a) adults and children, (b) men and women, (c) high and low socioeconomic status (SES) and (d) any particular combinations of the above?
3. How many times more likely were:
men to die than women, and
those of low SES to die than those of high SES?
4. To what historical event might these data refer?
Table 1.3 displays more complicated data than Table 1.2 because you had to consider the joint effects of three factors (sex, SES, and age) on mortality. The sequence of questions above underlines a general principle in describing such tables – i.e. to look at overall patterns first, then move on to more detail. We all see things in different ways, but until you develop your own style the approach shown in Box 1.2 may help you avoid getting lost in the array of possible relationships. You need first to grasp the size of the whole group under study and how many died; then check the overall patterns (the numbers and death rates1) across each ‘exposure’ separately (sex, SES, age). For example, first look at the death rates for all adult males, ignoring their SES, or for all people of high SES, ignoring their age and sex. Only then consider the more complex joint effects such as the influence of SES on mortality among women.
Things to note about the population include:
the predominance of adult males (1690 ÷ 2224 = 76%), the much smaller proportion of adult females (19%), and the very few children;
the substantial excess of persons of low SES (men and children in particular); and
the total population (2224) is quite large – a village, small town, an army barracks … ?
Things to note about the ‘death rates’ include the following.
The overall death rate is very high – more than two-thirds died.
Overall, death rates increased with decreasing SES.
The death rate in men (80.0%) was much higher than that in women (25.6%); the death rate in children was between these two.
In men, the death rate was high in all socioeconomic classes, although those of high SES fared better than the rest; in women, the death rate was always lower than that for males of equivalent SES, but it increased strikingly from high to medium to low SES.
The only children to die were of low SES.
Overall, the relative risk (RR) for men versus women is 80.0 ÷ 25.6 = 3.1
The RR for low versus high SES is 74.8 ÷ 37.5 = 2.0
The RR for women of low SES versus women of high SES is 53.9 ÷ 2.8 = 19.3
The RR for men of low SES versus women of high SES is 83.8 ÷ 2.8 = 29.9
A disaster has occurred, causing a high death rate that predominantly affected men (of all social classes) and, to a lesser extent, women and children of low social class. Overall there is a modest benefit of belonging to a higher social stratum, and among women this protection was exceptionally strong (a 19-fold higher risk of dying for low versus high SES).
Such substantial differences in risk reflect powerful preventive effects and in this instance it was a mix of social custom and the physical consequences of social stratification. The event was the sinking of the Titanic, where those of higher SES (the first-class passengers) were situated on the upper decks and were therefore closer to the lifeboats than those of medium and low SES (those travelling second and third class, respectively). The males gallantly helped the females and children into the lifeboats first. Those of ‘other’ SES were the crew.
In tackling this and the previous problem you have already done some serious epidemiology: you have described data, interpreted the patterns you observed and used epidemiological measures to help do this. We will build on this throughout the book, but first let’s step back a little and see what other lessons we can learn from the past.
The beginnings2
The ‘great man’ approach has fallen out of favour in modern historical practice; however, linking historical events to people adds character so we will focus on some of the main players in this brief overview of the development of population health and epidemiology.
Good epidemiological practice and reasoning started long ago. Perhaps the first proto-epidemiologist (proto because he did not actually count anything) was Hippocrates of Cos (460–375 BC), who recognised that both environmental and behavioural factors could affect health (see Box 1.3).
Whoever wishes to investigate medicine properly, should proceed thus: in the first place to consider the seasons of the year, and what effects each of them produces … Then the winds, the hot and the cold, especially such as are common to all countries, and then such as are peculiar to each locality. We must also consider the qualities of the waters … In the same manner, when one comes into a city to which he is a stranger, he ought to consider its situation, how it lies as to the winds and the rising of the sun; for its influence is not the same whether it lies to the north or the south, to the rising or to the setting sun. These things one ought to consider most attentively, and concerning the waters which the inhabitants use, whether they be marshy and soft, or hard, and running from elevated and rocky situations, and then if saltish and unfit for cooking; and the ground, whether it be naked and deficient in water, or wooded and well watered, and whether it lies in a hollow, confined situation, or is elevated and cold; and the mode in which the inhabitants live, and what are their pursuits, whether they are fond of drinking and eating to excess, and given to indolence, or are fond of exercise and labour …
The Dark Ages and Middle Ages (AD 500–1500) have little to say to us, other than in the development of causal reasoning, which we will set aside until later in the book (Chapter 10). The introduction of more quantitative methods into epidemiology and, in fact, into biology and medicine in general, has been attributed to John Graunt (1620–1674), a haberdasher and early Fellow of the Royal Society in London who published his Natural and Political Observations Mentioned in a Following Index and Made Upon the Bills of Mortality in 1662 (Graunt, 1662). He studied parish christening registers and the ‘Bills of Mortality’, and noted many features of birth and death data, including the higher numbers of both male births and deaths in comparison with females, the high rates of infant mortality and seasonal variations in mortality. He also provided a numerical account of the impact of the plague in London and made the first attempts to estimate the size of the population. In an attempt to define a ‘law of mortality’ he constructed the first life-table (Table 1.4). This summarised the health of a population in terms of the chance of an individual surviving to a particular age. Notice that at this time only three out of every hundred people reached the age of 66, and the majority of deaths occurred in early life. This technique was a forerunner of that used by life insurance companies for calculating insurance premiums today, as well as a fundamental approach to measuring a population’s health. As you will see, when we come back to consider life-tables in more detail in Chapter 2 (see also Appendix 5 for details of how to construct a life-table), things have improved considerably since Graunt’s time, with about 85 of every 100 men and 90 of every 100 women now making it to the age of 66 in developed countries.
| Exact age (years) | Deaths | Survivors | Chance of living to that age (%) |
|---|---|---|---|
| 0 | – | 100 | |
| 6 | 36 | 64 | 64 |
| 16 | 24 | 40 | 40 |
| 26 | 15 | 25 | 25 |
| 36 | 9 | 16 | 16 |
| 46 | 6 | 10 | 10 |
| 56 | 4 | 6 | 6 |
| 66 | 3 | 3 | 3 |
| 76 | 2 | 1 | 1 |
| 86 | 1 | 0 |
 More about some key figures
More about some key figures
During the nineteenth century, the collection and use of health statistics for what we now call ‘descriptive epidemiology’ continued to develop in England and also, briefly, in France. Of particular influence as a teacher was Pierre Charles-Alexandre Louis (1787–1872), who conducted some of the earliest epidemiological studies of treatment effectiveness when he demonstrated that bloodletting did not aid recovery from disease. Among his students was William Farr (1807–1883), physician, statistician and director of the Office of the Registrar General for England and Wales from 1837, its second year of operation. Farr studied levels of mortality in different occupations and institutions and in married and single persons, as well as other facets of the distribution of disease. He published these and other findings in the Annual Reports of the Registrar General, and the present UK system of vital statistics stems directly from his work.
 More about John Snow
More about John Snow
John Snow (1813–1858), a physician and contemporary of Farr, was better known at the time for giving chloroform to Queen Victoria during childbirth, but is now remembered for his pioneering work in elucidating the mode of transmission of cholera (Snow, 1855). This remains a classic and exciting example of epidemiological detection and some of Snow’s personal account of it is given below and again later in the chapter. His initial observations were based on a series of reports of individual cases of cholera and, in every instance, he was able to link the case to contact with another infected person (or their goods), thereby demonstrating that the disease could spread from person to person. He then surmised, contrary to popular belief at the time, that cholera could be transmitted through polluted water, a view that was strengthened by his observations linking a terrible outbreak of cholera around Broad Street, London, in 1854, to the local water pump (Box 1.4).
Within two hundred and fifty yards of the spot where Cambridge Street joins Broad Street, there were upwards of five hundred fatal attacks of cholera in ten days … The mortality would undoubtedly have been much greater had it not been for the flight of the population … so that in less than six days from the commencement of the outbreak, the most afflicted streets were deserted by more than three-quarters of their inhabitants.
There were a few cases of cholera in the neighbourhood of Broad Street, Golden Square, in the latter part of August; and the so-called outbreak, which commenced in the night between the 31st of August and the 1st of September, was, as in all similar instances, only a violent increase of the malady. As soon as I became acquainted with the situation and extent of this eruption of cholera, I suspected some contamination of the water of the much-frequented street-pump in Broad Street … but on examining the water … I found so little impurity in it of an organic nature, that I hesitated to come to a conclusion. Further inquiry, however, showed me that there was no other circumstance or agent common to the circumscribed locality in which this sudden increase of cholera occurred, and not extending beyond it, except the water of the above mentioned pump.
On proceeding to the spot, I found that nearly all the deaths had taken place within a short distance of the pump. There were only ten deaths in houses situated decidedly nearer to another street pump. In five of these cases the families of the deceased persons informed me that they always sent to the pump in Broad Street, as they preferred the water to that of the pump which was nearer. In three other cases, the deceased were children who went to school near the pump in Broad Street. Two of them were known to drink the water; and the parents of the third think it probable that it did so. The other two deaths, beyond the district which this pump supplies, represent only the amount of mortality from cholera that was occurring before the irruption took place … [Snow used a spot map to show the spread of cases in relation to this and other pumps.] I had an interview with the Board of Guardians of St James’s parish, on the evening of Thursday, 7th September, and represented the above circumstances to them. In consequence of what I said, the handle of the pump was removed on the following day.
Snow was also able to explain why some groups of people within the area did not develop cholera:
The Workhouse in Poland Street is more than three-fourths surrounded by houses in which deaths from cholera occurred, yet out of five hundred and thirty-five inmates, only five died of cholera, … The workhouse has a pump well on the premises, … and the inmates never sent to Broad Street for water. If the mortality in the workhouse had been equal to that in the streets immediately surrounding it on three sides, upwards of one hundred persons would have died. [Note Snow’s comparison of the ‘observed’ number of cases with the number ‘expected’.]
There is a Brewery in Broad Street, near to the pump, and on perceiving that no brewery men were registered as having died of cholera, I called on Mr Huggins, the proprietor. He informed me that there were above seventy workmen employed in the brewery, and that none of them had suffered from cholera … The men are allowed a certain quantity of malt liquor, and Mr Huggins believes they do not drink water at all …
The limited district in which this outbreak of cholera occurred, contains a great variety in the quality of the streets and houses; Poland Street and Great Pulteney Street consisting in a great measure of private houses occupied by one family, whilst Husband Street and Peter Street are occupied by the poor Irish. The remaining streets are intermediate in point of respectability. The mortality appears to have fallen pretty equally amongst all classes, in proportion to their number.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


