14 Endocrinology and Diabetes
Diabetes mellitus
The likelihood is that this patient has type 2 diabetes (Table 14.1). The risk of ketoacidosis is small and he will not need admission unless he is either ketotic (ketonuria 3+) or is very dehydrated.
Table 14.1 The spectrum of diabetes: a comparison of type 1 and type 2 diabetes mellitus
| Type 1 | Type 2 | |
|---|---|---|
| Epidemiology | Younger (usually < 30 years of age) | Older (usually > 30 years of age) |
| Usually lean | Often overweight | |
| Increased in those of Northern European ancestry | All racial groups. Increased in peoples of Asian, African, Polynesian and American-Indian ancestry | |
| Seasonal incidence | ||
| Heredity | HLA-DR3 or DR4 in > 90% | No HLA links |
| 30–50% concordance in identical twins | ~ 50% concordance in identical twins | |
| Pathogenesis | Autoimmune disease | No immune disturbance |
| Islet cell autoantibodies | Insulin resistance | |
| Insulitis | ||
| Association with other autoimmune diseases | ||
| Immunosuppression after diagnosis delays beta-cell destruction | ||
| Clinical | Insulin deficiency | Partial insulin deficiency initially |
| May develop ketoacidosis | May develop hyperosmolar state | |
| Always need insulin | Many come to need insulin when beta-cells fail over time | |
| Biochemical | Eventual disappearance of C-peptide | C-peptide persists |
Note: there is a significant rise in the incidence of young patients with type 2 diabetes mellitus, especially in the obese and in Asian populations.
Indications for admission
Information
Diagnostic criteria for diabetes mellitus:
• Fasting venous plasma glucose > 7.0 mmol/L (126 mg/dL) after 8-h fast*
• Random venous plasma glucose > 11.1 mmol/L (200 mg/dL)*
• An HbA1c of > 6.5% (48 mmol/mol) has recently been approved for diagnosis (Table 14.2)
• Impaired fasting glucose: 5.6–6.9 mmol/L
• Impaired glucose tolerance: > 7.8 and < 11.1 mmol/L; 2 h after 75 g oral GTT.
Table 14.2 HBA1c – conversion of percentage values to mmol/mol
| DCCT HbA1c % | IFCC HbA1c mmol/mol |
|---|---|
| 4.0 | 20 |
| 5.0 | 31 |
| 6.0 | 42 |
| 6.5 | 48 |
| 7.0 | 53 |
| 7.5 | 59 |
| 8.0 | 64 |
| 9.0 | 75 |
| 10.0 | 96 |
DCCT, Diabetes control and complication trial.
IFCC, International Federation of Clinical Chemistry.
An oral glucose tolerance test is only required for borderline cases.
Progress.
This patient is much more likely to be presenting with early type 1 diabetes and might not be ketotic yet because he could still have a degree of residual beta cell function (the ‘honeymoon’ phase). Again, assessment of ketosis, acidosis and dehydration must be made to determine whether he needs admission. He should be seen within 24 h either by the diabetic liaison nurse or in hospital to commence insulin. If there is any doubt, the patient should be seen in A&E immediately.
Diabetic ketoacidosis (DKA)
How do patients present with ketoacidosis?
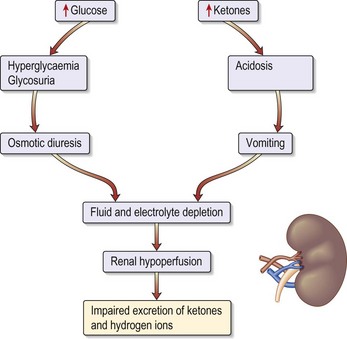
Patients known to have type 1 diabetes mellitus most commonly develop ketoacidosis when insulin is omitted because of missed meals during an intercurrent illness (e.g. gastroenteritis). Patients become rapidly dehydrated (Fig. 14.1) and acidotic (over hours). Tachypnoea or Kussmaul respiration (a deep sighing respiration) is prominent, with the smell of ketones on the breath. It is the fall in pH that causes coma.
Assessment of severity
Poor prognostic features include:
Management: general measures
• Insert a central line in patients with a history of cardiac disease/renal impairment/autonomic neuropathy or the elderly.
• An arterial line to monitor ABGs and plasma potassium.
• Nil by mouth for at least 6 h.
• Nasogastric tube: if there is impaired conscious level, to prevent vomiting and aspiration.
• Urinary catheter: if no urine for 2 hours or serum creatinine is high.
Management: fluid replacement
Severely shocked patients may require colloid to restore circulating plasma volume. Table 14.3 shows examples of blood values in severe ketoacidosis and compares these with those seen in the hyperosmolar, hyperglycaemic state described on page 418.

The guidelines for fluid replacement are shown in Table 14.4. These are applicable for young patients.
• When blood glucose falls to less than 12 mmol/L convert to a 5% glucose infusion. This will enable the insulin infusion to be continued. Continued insulin is required to inhibit ketone production.
• Continue with IV fluids 1 L every 4–6 h until rehydrated and ketosis resolves (~24 h).
Table 14.4 Guidelines for average fluid replacement in young patients
| Volume | Duration/timing |
|---|---|
| 1 L 0.9% saline + 20 mmol/KCl | Over the first 30 min |
| 1 L 0.9% saline + 20 mmol/KCl | Over next 1 h |
| 1 L 0.9% saline + 20 mmol/KCl | Over next 2 h |
| 1 L 0.9% saline + 20 mmol/KCl | Over next 4–6 h |
Management: insulin regimen
• Add 50 units of soluble insulin to 50 mL 0.9% saline and administer by intravenous infusion; this equates to 1 U/mL.
• Commence at 6 U/h and continue at 3 U/h after venous glucose falls to < 11.5 mmol/L.
• Glucose must then be administered to prevent hypoglycaemia (see above).
• Continue IV insulin infusion until ketosis resolves, the patient is eating and for 2–4 h after the first SC dose of soluble insulin.
Management: potassium replacement (Table 14.5)
• Monitor serum [K+] every 2 h initially then every 4 h until stable.
• Use premixed potassium-containing infusions wherever possible.
Table 14.5 Potassium replacement in patients with diabetic ketoacidosis
| Serum potassium (mmol/L) | Amount of KCl (mmol/hour) |
|---|---|
| <3 | 40 |
| 3–1 | 30 |
| 4–5 | 20 |
| 5–6 | 10 |
| > 6 | Stop KCl |
Assessment during treatment
• Remember the role of insulin is primarily to suppress ketogenesis rather than to lower blood glucose.
• Blood glucose (BM Stix every hour, laboratory blood glucose 4-hourly).
• Plasma potassium every 4 h: the main risk is hypokalaemia.
• Repeat ABGs after 2 h. A calculated anion gap (needs chloride estimation) may be adequate for monitoring.
Hyperosmolar hyperglycaemic state
How do patients present?
Diagnosis and investigations
• Plasma glucose: usually > 40 mmol/L.
• U&Es: significant hypernatraemia occurs but this is masked by the high glucose. The [Na+] usually increases as the venous glucose and therefore the extracellular colloid osmotic pressure falls and water moves into the intracellular space.
• Arterial blood gases: relatively normal.
• Plasma osmolality: typically > 350 mOsmol/kg.
• Estimate corrected sodium to evaluate water loss as a result of hyperglycaemia (see Information box).
• FBC: may show polycythaemia, dehydration or a leucocytosis from infection.
• CK: cardiac ischaemia or rhabdomyolysis.
• ECG: for myocardial infarction or ischaemia.
• CXR: for signs of infection.
How would you manage this patient?
General treatment measures
• Aim to correct the high osmolality with fluid and insulin over 48–72 h. Avoid fluid overload and insert a central venous line if cardiac problems.
• When blood glucose is less than 10 mmol/L, commence a 5% glucose infusion.
• Once stable, stop insulin therapy and commence oral hypoglycaemic agents or diet alone.
Hypoglycaemic coma
How do patients present? (Table 14.6)
Table 14.6 Presentation of patients with hypoglycaemic coma
| Sympathetic overactivity (glucose < 3.5 mmol/L) | Neuroglycopenia (glucose < 2.6 mmol/L) |
|---|---|
| Tachycardia | Confusion |
| Palpitations | Slurred speech |
| Sweating | Localised neurological impairment |
| Anxiety | Coma |
| Pallor | |
| Tremor | |
| Cold extremities |
Assessment of severity
• Hypoglycaemia in a patient with diabetes is defined as < 3.5 mmol/L.
• A ‘mild’ episode requires intervention by the patient.
• A ‘severe’ episode might lead to coma and requires treatment by a third party.
Investigations
Patients with diabetes with frequent hypoglycaemic attacks:
• Urea and electrolytes: hypoglycaemia is more common in diabetic nephropathy because the kidney is one of the sites of insulin metabolism
• Thyroid function tests: hypothyroidism is associated with type 1 diabetes mellitus and impairs counter-regulation
• 09:00 cortisol ± short ACTH (tetracosactide) stimulation test: hypoadrenalism reduces hepatic glycogen stores (see p. 443)
How would you manage hypoglycaemia?
Unconscious patient
• Do not use 50% glucose in peripheral veins.
• Once recovered, give 1–2 slices of bread or 2–4 biscuits.
• Admit the patient if the cause is a long-acting sulphonylurea or a long-acting insulin and give a continuous infusion of 10% glucose (e.g. 1 litre 8-hourly) and check glucose hourly or 2-hourly.
• Patients should regain consciousness or become coherent within 10 min, although complete cognitive recovery might lag by 30–45 min. Do not give further boluses of IV glucose without repeating the blood glucose. If the patient does not wake up after 10 min or more, repeat the blood glucose and consider another cause of coma – stroke or a head injury during their confused state.
Sick diabetic patient
Treatment/progress
This patient has a diagnosis of STEMI and requires immediate therapy with aspirin 300 mg chewed and clopidogrel 300 mg oral gel. He was immediately transferred to the Coronary Care Unit for further assessment and possible percutaneous coronary intervention, which is instantly available (p. 285). His diabetes was initially controlled on insulin infusion because he was nil by mouth for the cardiac procedures (Table 14.7). The infusion was continued until the patient was eating and drinking. Insulin treatment has been proven to improve outcome in patients with diabetes in the immediate period after myocardial infarction.
Table 14.7 Intravenous infusion insulin management of type 1 diabetes mellitus in hospital
| Level of blood glucose (measured hourly) | Insulin infusion (units per hour) |
|---|---|
| < 4.0 mmol/L | 0.5 |
| 4.0–7.0 mmol/L | 1 |
| 7.1–9.0 mmol/L | 2 |
| 9.1–11.0 mmol/L | 3 |
| 11.1–14.0 mmol/L | 4 |
| 14.1–17.0 mmol/L | 5 |
| 17.1–28 mmol/L | 6 |
| > 28 mmol/L | 8 |
Note: the above is only a guide and insulin doses should be adjusted upwards if the patient is known to have a high insulin requirement, and always reviewed regularly to see if the doses are appropriate. The aim is to keep blood glucose in the 7–9 region.
Protocol for converting diabetics from intravenous to subcutaneous insulin
• Calculate total dose over last 24 h.
• Give 25% of total as soluble insulin 30 min before each meal (i.e. × 3 daily).
• Give 25% of total dose as intermediate-acting isophane insulin at 22:00.
• Monitor blood glucose fasting and 2 h after meals (post-prandial) – each finger-prick glucose measures the adequacy of the previous dose.
• Aim for glucose < 10 mmol/L post-prandial and < 8 mmol/L fasting.
• Do not discontinue IV insulin until 1–2 h after the first subcutaneous insulin dose is administered, because IV insulin has a half-life of only 3 min.
Management of new type 2 diabetic presenting for surgery
How would you manage this patient?
• Ask about symptoms of diabetes, e.g. thirst, polyuria, lack of energy.
• Check that a laboratory glucose has been sent to confirm the diagnosis of diabetes (random glucose 13.4 mmol/L).
• Discuss patient’s angina symptoms and discuss with cardiologist the urgency of CABG surgery.
• It is agreed by all, including the patient, that his diabetes should be treated and blood sugar controlled before surgery is performed.
• The patient is referred to the Diabetic Liaison Nurse for assessment and discussion of treatment as an outpatient.
Remember
Always get diabetes under control before patients undergo surgery unless this is an emergency.
Information
Assessment of new patients with diabetes
• Biochemical assessment of long-term glycaemic control (e.g. HbA1c)
• Examine the retina through dilated fundi (ophthalmoscope initially followed by retinal photo)
• Test blood for renal function (creatinine and eGFR)
• Check general condition of the feet, peripheral pulses and sensation
• Review cardiovascular risk factors
• Introduce self-monitoring and injection techniques if insulin is required
Management for surgery
Non-insulin-treated patients should stop medication 2 days before the procedure. Patients with mild hyperglycaemia (fasting blood glucose < 8 mmol/L) can be treated as non-diabetic. Those with higher levels are treated with soluble insulin prior to the procedure/surgery, and with glucose, insulin and potassium infusion during and after the procedure (p. 426). Be careful of hypoglycaemia due to the additive effect of medications taken previously. Postoperatively, patients should return to their normal management regimen when they begin eating and drinking.
Who needs insulin perioperatively?
• All patients who usually use insulin
• All acute surgical emergencies (type 1 and type 2 diabetes)
• All patients undergoing major surgery (type 1 and type 2 diabetes).
In other words, all diabetic patients should receive insulin except type 2 diabetic subjects undergoing minor surgery. For patients on insulin, give the usual evening and/or night-time insulin and commence glucose and insulin as above at 06:00.
Urgent surgery in patients with diabetes
The procedure for insulin-treated patients is simple:
Preoperative glucose levels should be in the range of 7–11 mmol/L.
Postoperatively, the infusion is maintained until the patient is able to eat. Other fluids needed in the perioperative period must be given through a separate IV line and must not interrupt the glucose/insulin/potassium infusion. Glucose levels are checked every 2–4 hours and potassium levels are monitored. The amount of insulin and potassium in each infusion bag is adjusted either upwards or downwards according to the results of regular monitoring of the blood glucose and serum potassium concentrations.



