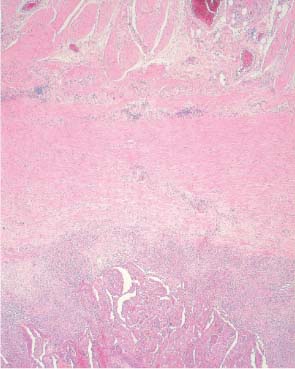
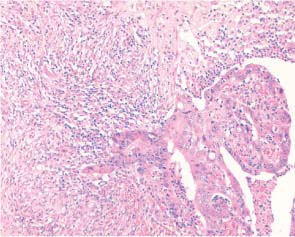
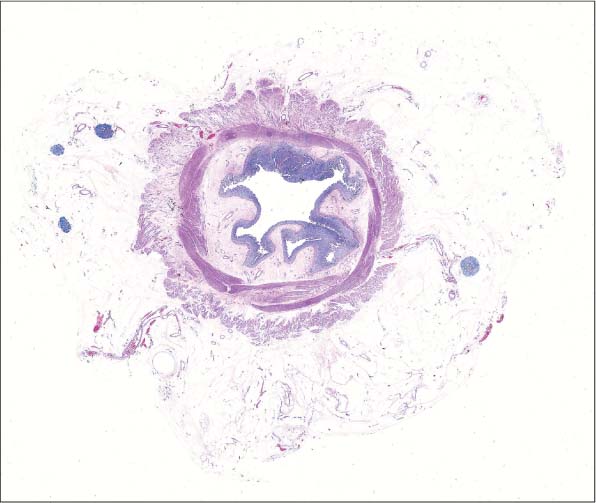
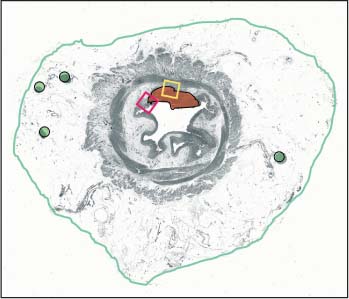
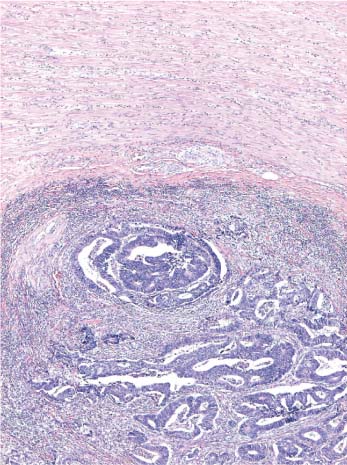
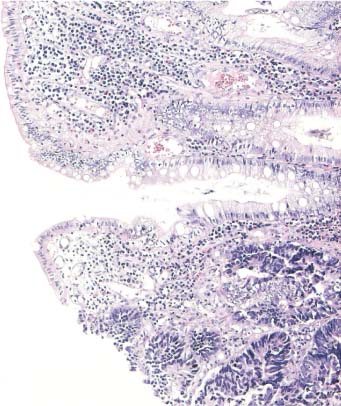
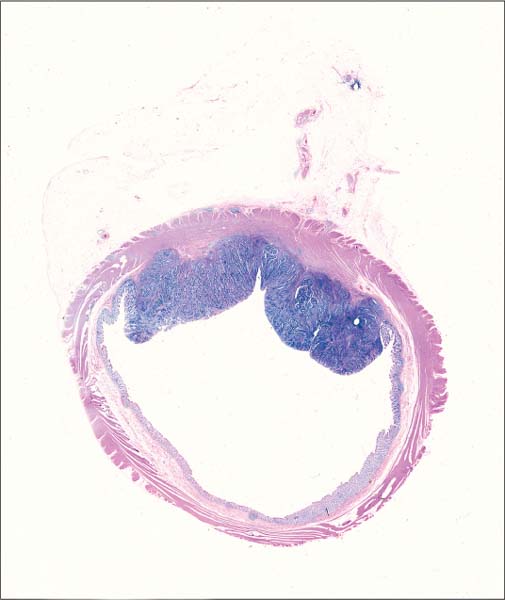
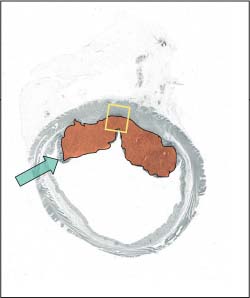
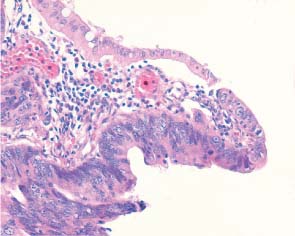
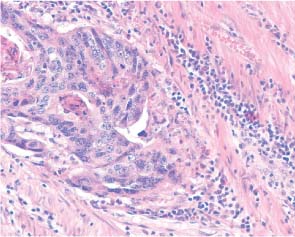
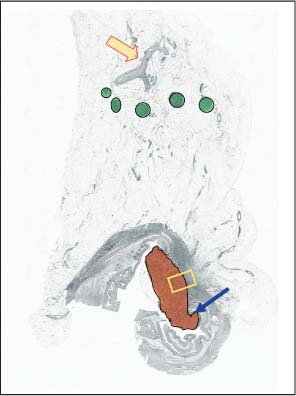
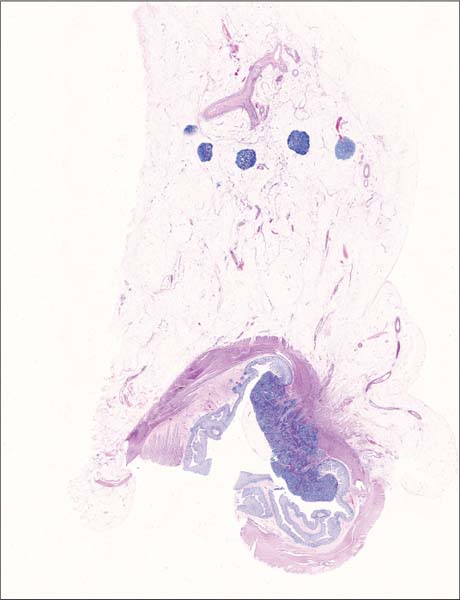
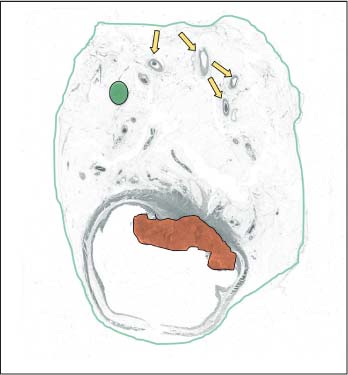
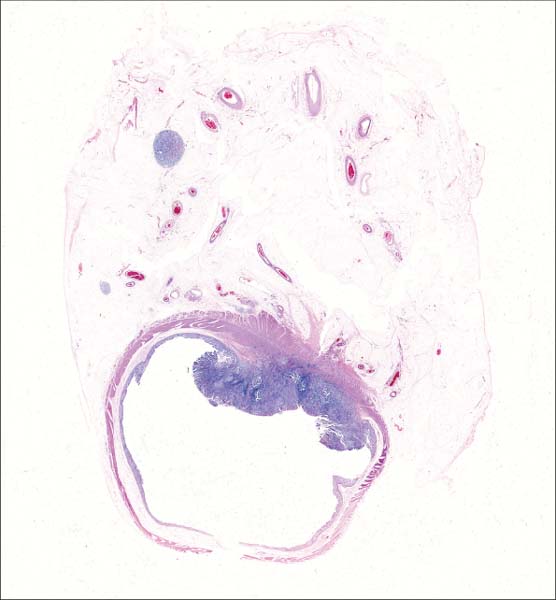
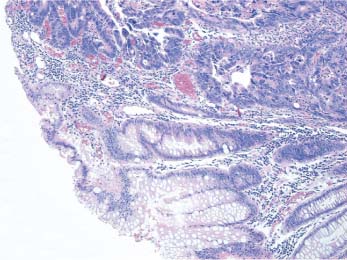
2 Early Colorectal Cancer Patient data: 65-year-old woman with rectal pain. Endoscopically, a small suspicious lesion was found 7 cm from the anus. A preoperative diagnosis of invasive carcinoma was made on endoscopic biopsy. Surgical treatment: Mesorectal resection, no preoperative irradiation. Specimen: 22-cm-long rectum with an exophytic tumor 15 mm in diameter, 1cm from the distal margin. Histopathologic diagnosis: Moderately differentiated rectal adenocarcinoma infiltrating into the submucosa and reaching the inner layer of the lamina muscularis propria, 13 lymph nodes without signs of metastasis, radical excision, mesorectal margin 22 mm. TNM stage: I (T2N0M0), Dukes A. Follow-up: 12 months, no signs of disease recurrence. The level of the deepest invasion of the tumor and the presence or absence of metastasis are the most important prognostic factors in colorectal cancer. Tumors without metastasis and confined to the bowel wall (corresponding to stage A in Dukes’ system or to one of the categories T1 or T2 in the TNM classification) have a good prognosis and may be designated as early colorectal cancer. Thus, proper assessment of the deepest level of tumoral invasion is crucial for adequate staging of the disease. The early rectal cancer in the presented case infiltrated only the submucosa of the rectum. As demonstrated in Figure 2.1, the tumor (corresponding to the red-colored area in the schematic image, Fig. 2.1d) just touched the inner muscular layer while the rest of the lamina muscularis propria remained intact. The abrupt transition from normal mucosa to neoplastic tissue, shown in Figure 2.1a (a microscopic magnification of the area of the red rectangle in Fig. 2.1d), indicates that this tumor may have developed without a precancerous stage of adenoma. The deepest level of infiltration (corresponding to the yellow rectangle in Fig. 2.1d) is microscopically magnified in Figure 2.1b. Further magnification of the same structures is seen in Figure 2.1c. As marked with the green colored circles in the schematic image, the large section contained four perirectal lymph nodes, which were free of metastasis. A continuous circumferential surgical margin (green-lined periphery of the specimen in Fig. 2.1d) is also shown; its distance to the nearest level of invasion is easy to assess. Fig. 2.1a Fig. 2.1b Fig. 2.1c Fig. 2.1 Large-section histology image of an early carcinoma of the rectum. Fig. 2.1d Schematic guide to the morphologic details in the large section in Fig. 2.1. Patient data: 82-year-old man with rectal bleeding. Endoscopically, a 4 × 3-cm suspicious lesion was seen 13 cm from the anus. A preoperative diagnosis of invasive carcinoma was made on endoscopic biopsy. Surgical treatment: Rectosigmoidal resection, no preoperative irradiation. Specimen: 20-cm-long rectosigmoideum with a 4 ×3-cm exophytic tumor, 5 cm from the distal margin. Histopathologic diagnosis: Moderately differentiated rectal adenocarcinoma infiltrating in but not beyond the lamina muscularis propria, 8 lymph nodes without signs of metastasis, radical excision, mesorectal margin 20 mm. TNM stage: I (T2N0M0), Dukes A. Follow-up: The patient died of heart failure 38 months after operation, without signs of recurrence of the tumor. The exophytic tumor presented in Figure 2.2 is an early invasive carcinoma infiltrating in but not through the lamina muscularis propria. The area of the tumor is colored red in the schematic image (Fig. 2.2d). The level of infiltration in the muscularis propria is very well seen in the large histologic section. The deepest level of invasion is microscopically magnified in Figure 2.2a (corresponding to the area of the yellow rectangle in Fig. 2.2d). The level of infiltration – far beyond the lamina muscularis propria is easy to assess. Tumors operated at this early stage of development of rectal carcinoma have an excellent prognosis. Based on the abrupt transition of the normal epithelium into the tumor tissue, illustrated in Figure 2.2b (corresponding to the area marked with the green arrow in Fig. 2.2d), one may assume that the tumor, similar to the one discussed in the previous case, had developed without a stage of preexisting adenoma. These tumors, sometimes called „flat adenocarcinomas of the colorectum“ may have a poorer prognosis than their „polypoid“ counterparts, which develop through a precancerous stage of adenoma (Nasir et al. 2004). Fig. 2.2a Fig. 2.2b Fig. 2.2 Large-section histology image of an early carcinoma of the rectum. Fig. 2.2c Schematic guide to the morphologic details in the large section in Fig. 2.2. Patient data: 85-year-old man presenting with rectal bleeding. Endoscopically, a small polypoid lesion was found in the sigmoideum. A preoperative diagnosis of invasive carcinoma was made on endoscopic biopsy. Surgical treatment: Sigmoideum resection, no preoperative irradiation. Specimen: 11-cm-long sigmoideum with an exophytic tumor 20mm in diameter, 4 cm from one of the margins. Histopathologic diagnosis: Moderately differentiated adenocarcinoma infiltrating into but not beyond the lamina muscularis propria, 10 lymph nodes without signs of metastasis, radical excision. TNM stage: I (T2N0M0), Dukes A. Follow-up: 20 months, without signs of recurrence of colon carcinoma. The patient developed prostate cancer, diagnosed 10 months after surgery for colon cancer. The large histologic section in Figure 2.3 reliably demonstrates the level of invasion of the colon carcinoma (the tumor corresponds to the red-colored area in the schematic image, Fig. 2.3c), not reaching the outer layer of the lamina muscularis propria. The zone of transition between normal and neoplastic epithelium is illustrated in Figure 2.3a (microscopy image of the detail marked with the blue arrow in Fig. 2.3c). The deepest level of invasion corresponds to the area of the yellow rectangle in Figure 2.3c (microscopically magnified in Fig. 2.3b). The large section also included 5 lymph nodes free of metastasis (marked with green circles in Fig. 2.3c). The yellow arrow in Figure 2.3c indicates the mesenterial artery, the „root“ of the surgical specimen. Fig. 2.3a Fig. 2.3b Fig. 2.3c Schematic guide to the morphologic details in the large section in Fig. 2.3. Fig. 2.3 Large-section histology image of an early colon carcinoma. Patient data: 70-year-old man presenting with rectal bleeding. Endoscopically, a small polypoid lesion was found in the rectum, 10 cm from the anus. A preoperative diagnosis of invasive carcinoma was made on endoscopic biopsy. Surgical treatment: mesorectal resection, no preoperative irradiation. Specimen: 18-cm-long rectum with an exophytic tumor 30mm in diameter, 5cm from the distal margin. Histopathologic diagnosis: Moderately differentiated adenocarcinoma infiltrating into but not beyond the lamina muscularis propria, 12 lymph nodes without signs of metastasis, radical excision. TNM stage: I (T2N0M0), Dukes A. Follow-up: 54 months, no signs of disease recurrence. This rectal carcinoma had obviously developed in an adenoma and infiltrated through the inner layer of the lamina muscularis propria into the outer layer, without reaching the perirectal tissue (Fig. 2.4). The tumor is marked with the red-colored area in the schematic image (Fig. 2.4a). Note the negative lymph node marked with green circle in Figure 2.4a. The specimen also included branches of the mesenteric artery (marked with yellow arrows in Fig. 2.4a). The circumferential margin, corresponding to the green-colored periphery of the schematic image, is well seen in the large histologic section and can be easily analyzed in all directions: at the lower edge, corresponding to the peritonealized ventral surface of the rectum, as well as at the upper part, corresponding to the surgical mesorectal margin. Fig. 2.4a Schematic guide to the morphologic details in the large section in Fig. 2.4. Fig. 2.4 Large-section histology image of an early rectal carcinoma. Patient data: 85-year-old man presenting with rectal bleeding. Endoscopically, a small polypoid lesion was found in the rectum, 7 cm from the anus. A preoperative diagnosis of invasive carcinoma was made on endoscopic biopsy. Surgical treatment: Rectosigmoidal resection, no preoperative irradiation. Specimen: 20-cm-long rectosigmoideum with a 5 ×3-cm ulcerated tumor, 2 cm from the distal margin. Histopathologic diagnosis: Moderately differentiated adenocarcinoma infiltrating into but not beyond the lamina muscularis propria, 16 lymph nodes without signs of metastasis, radical excision. TNM stage: I (T2N0M0), Dukes A. Follow-up: 8 months, no signs of disease recurrence. This large histologic section (Fig. 2.5) demonstrates an early carcinoma in the rectum infiltrating the lamina muscularis propria up to the border between the inner and outer muscle layers. The tumor destroyed about one half of the circumference of the mucosal surface. Note the lymph node in the mesorectum and the well-represented circumferential resection margin. The area of transition between the normal mucosa and the periphery of the tumor is magnified in Figure 2.5a (corresponding to the yellow-colored rectangle in the schematic image, Fig. 2.5d). Figure 2.5b represents a further detail of the invasive cancer in the same area. The deepest level of invasion was found in the area of the red rectangle in Figure 2.5d (microscopically magnified in Fig. 2.5c). The green arrow in Figure 2.5d marks the distance between the deepest level of invasion and the surgical margin (orange-colored in Fig. 2.5d), corresponding to the mesorectal resection margin. A free mesorectal resection margin has been found to be of crucial importance for proper surgical management of rectal cancers and for lowering the frequency of local recurrences. Thus, proper assessment of the distance indicated with the green arrow in Figure 2.5d is one of the most important tasks in modern surgical pathology.
Case 2.1 Early Carcinoma of the Rectum
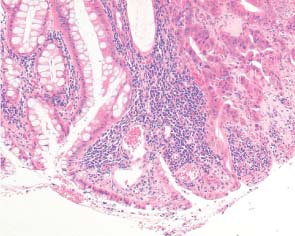
Practical points
Case 2.2 Early Carcinoma of the Rectum
Practical points
Case 2.3 Early Colon Carcinoma, Dukes A
Practical points
Case 2.4 Early Rectal Carcinoma, Dukes A
Practical points
Case 2.5 Early Rectal Cancer
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


