Drugs Used for Skin Disorders
Overview
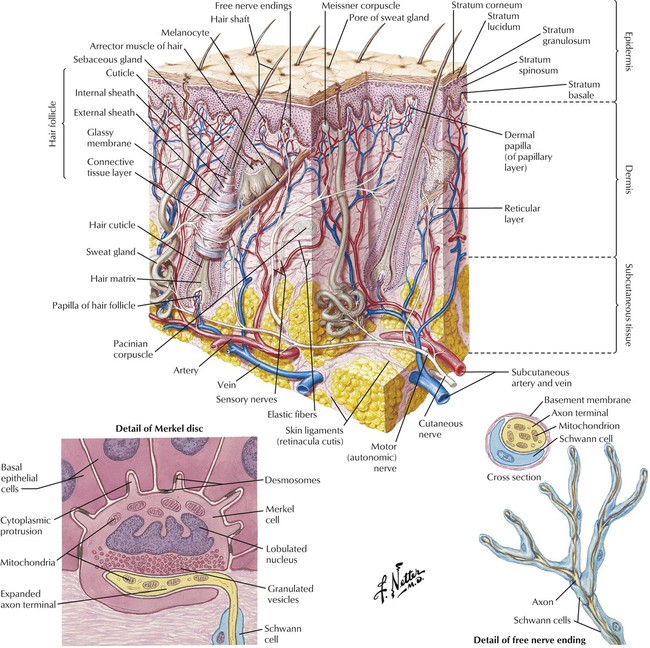
The skin is a complex, multicomponent organ. It is commonly classified into 3 anatomical regions and multiple subregions: the epidermis, which includes the strata corneum, lucidum, granulosum, spinosum, and basale; the dermis, which includes the papillary and reticular layers; and the subcutaneous tissue, which includes sweat glands. All layers are extensively supplied by blood vessels and innervated by motor and sensory neurons. Disorders of the skin can develop either as primary disease (localized to 1 or more layers of the skin) or as a secondary result of a systemic disease. Drugs for management of these disorders involve topical or systemic administration of medications to treat the dermal or systemic source of the problem. Major classes of drugs used in dermatologic pharmacology include glucocorticoids, antibacterials, antifungals, antivirals, antiparasitics, and retinoids.
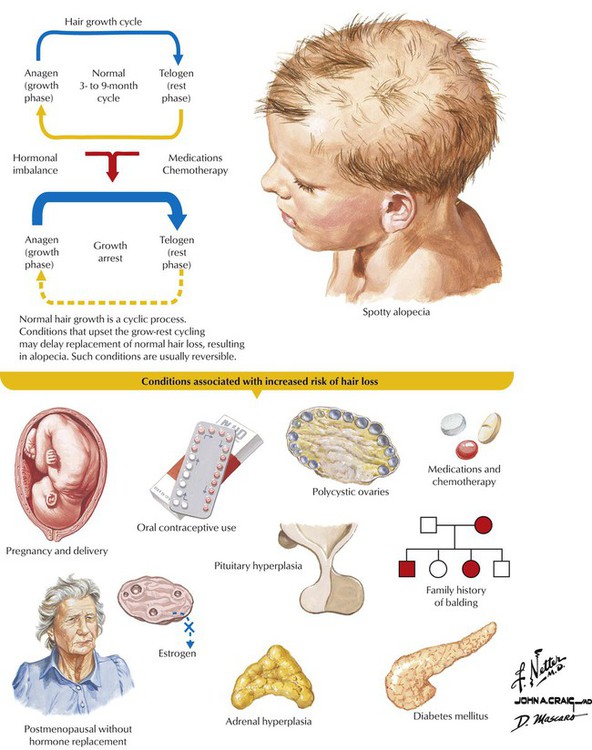
Alopecia—the loss or absence of hair, especially of the head—can be caused by illness, drugs, endocrine disorders, some types of dermatitis, hereditary factors, radiation, and physiologic processes such as aging. Drug therapy, when appropriate, involves topical steroids (eg, clobetasol) or intradermal injections of triamcinolone for alopecia areata (defined patches, usually on the scalp or beard; occurs most often in children and in autoimmune diseases); minoxidil for androgenic alopecia (affects androgen-sensitive follicles on the scalp of men and women); and griseofulvin, itraconazole, or terbinafine for tinea capitis (fungal infection). Scarring (cicatricial) and permanent alopecias are treated with potent corticosteroids used topically or intralesionally on active inflammatory borders. Systemic drugs (eg, acitretin, chloroquine, doxycycline, low-dose methotrexate, minocycline, prednisone, quinacrine, tetracyclines) may also be used if the disease type and extent warrant them.![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


