6 Dosage and dosage forms in herbal medicine
Chapter contents
The subject of appropriate dose is probably the most controversial aspect of contemporary Western herbal medicine. Among Western herbal practitioners, many different dosage approaches are found from country to country and within countries. Underlying these different approaches are different philosophies about the therapeutic action of medicinal plants.
• dosage ranges used in other important herbal traditions, e.g. China and India
• dosages used by important historical movements in Western herbal medicine, e.g. the Eclectics
• dosages currently recommended in pharmacopoeias
• dosages established from pharmacological and clinical research.
Review of dosage approaches
Traditional Chinese medicine
The daily dose for individual non-toxic herbs in traditional Chinese medicine is usually in the range of 3 to 10 g, given as a decoction or in pill or powder form.1 Often higher doses are prescribed by decoction than for pills, as might be expected since not all active components readily dissolve in hot water.2 (Pills generally consist of the powdered herb incorporated into a suitable base.) Herbs are invariably prescribed in formulations. Doses for such formulations are about 3 to 9 g taken three times daily but can be higher in the case of decoctions.
For each individual herb, a wide dosage range is usually given in texts. (This applies for all herbal systems.) One reason for this is that if a herb is used by itself or with just a few other herbs, a larger dose is used than when it is combined with many other herbs.2 Dose also varies according to the weight and age of patients and the severity or acuteness of their condition.
Some herbs, or closely related species, are used in both Chinese and Western herbal medicine. Table 6.11,3,4 compares dosages for a few of these herbs.
Table 6.1 Comparison of dosages used in Chinese and Western herbal medicine
| Herb | Chinese dosage1 g/day | Western dosage3,4 g/day |
|---|---|---|
| Ephedra sinica | 3–9 | 3–9 (extract) |
| 3–12 (decoction) | ||
| Zingiber officinale | 3–9 | 0.75–3 (decoction) |
| 0.38–0.75 (tincture) | ||
| Taraxacum mongolicum | 9–30 | 6–24 (decoction) |
| 3–6 (tincture) | ||
| Glycyrrhiza uralensis | 3–12 | 3–12 (decoction) |
| 6–12 (extract) | ||
| Rheum palmatum | 3–6 | 2.3–4.5 (decoction) |
| 1.8–6 (extract) |
Note: For dosages of tinctures and extracts given three times daily, the corresponding amount of dried herb per day has been calculated.
Ayurveda
Ayurveda often involves complex formulations which are prepared over several days and can contain many herbal and mineral components. Consequently, there is more dosage diversity than for Chinese medicine. Dosage ranges for individual non-toxic herbs are generally in the region of 1 to 6 g/day as powders or tinctures, with higher doses often recommended for decoctions.5
Eclectic medicine
Eclectic medicine was a largely empirical school of medicine which developed in America during the 19th century.6 The movement was most prominent for a brief period from the late 19th to the early 20th centuries, when there were several teaching universities and many eminent scholars in the USA. Although the Eclectics used simple chemical medicines such as phosphoric acid, they mainly prescribed herbal medicines. Their knowledge of materia medica was their greatest contribution to Western herbal medicine; for example, herbs such as Echinacea and golden seal were made popular by them after observation of their use by the Native Americans.
The Eclectics tended to use higher doses than those recommended in current texts and pharmacopoeias, although the ranges tend to overlap. Table 6.2 compares dosages currently used3,4 with those found in Eclectic texts7,8 for alcoholic extracts of herbs.
Table 6.2 Comparison of dosages used by the Eclectics and modern dosages
| Herb | Eclectic dosage7,8 g/day | Current dosage3,4 g/day |
|---|---|---|
| Euphorbia hirta | 1.8–10.8 | 0.36–0.9 |
| Echinacea angustifolia | 0.9–5.4 | 0.75–3.0 |
| Hydrastis canadensis | 0.9–10.8 | 0.9–3.0 |
| Passiflora incarnata | 1.8–10.8 | 1.5–3.0 |
| Valeriana officinalis | 2.1–6.0 | 0.9–3.0 |
| Rumex crispus | 1.8–10.8 | 6.0–12.0 |
| Viburnum opulus | 3.6–10.8 | 6.0–12.0 |
| Serenoa repens | 2.7–10.8 | 1.8–4.5 |
Note: The corresponding amount of dried herb per day has been calculated from recommended dosages for fluid extracts.
The British Herbal Pharmacopoeia
The British Herbal Pharmacopoeia 1983 (BHP) carries extensive dosage information for individual herbs and is generally regarded as an important traditional reference on this subject for Western herbal practitioners. Dosages given in the BHP were derived from earlier texts such as the British Pharmacopoeia (BP) and the British Pharmaceutical Codex (BPC) but also resulted from a survey of herbal practitioners. More recently, the British Herbal Compendium (BHC) has been published in two volumes, with dosage information for the practitioner.9,10
The doses given by the BHP 1983 contain some inconsistencies. The main problem is that doses for tinctures often do not correlate to corresponding doses for liquid extracts. For a 1:1 extract and a 1:5 tincture of a particular herb to correlate in terms of dose, the dose range for the tincture should be five times that of the extract, since it is theoretically five times weaker. This problem contrasts with other pharmacopoeias such as the BPC 1934 where the correlation is generally, but not exactly, observed. Some examples that highlight this problem are provided in Table 6.3.
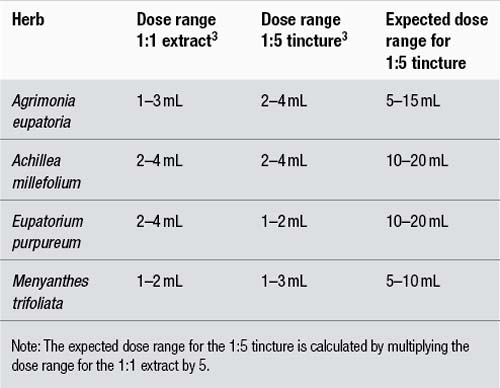
The poor correlation demonstrated in Table 6.3, where in the case of Eupatorium purpureum the tincture dose is actually less than the extract dose, probably arises for two reasons:
1. As stated above, the BHP 1983 doses were in part derived from a survey of herbal practitioners. It is probable that there were different dosage philosophies between practitioners using extracts compared to those using tinctures. Hence, a correlation should not be expected.
2. Tinctures are manufactured using different techniques to 1:1 fluid extracts. This is particularly important. Fluid extracts can be prepared by reconstituting more concentrated extracts, rather than the traditional method of reserved percolation. In either case, the heat or vacuum used in concentration can rob the preparation of important active chemicals. Tinctures better preserve the activity of the whole plant because they are made without heat or a concentration procedure. Fluid extracts were also often manufactured using lower alcohol strengths than tinctures, and important active components may therefore not be extracted from the starting plant material. The result of these factors is that a 1:1 fluid extract can have an activity which is much less than five times that of a 1:5 tincture. This will be dealt with in more detail in the part of this chapter that discusses liquid preparations.
Commission E and ESCOP monographs
A positive monograph for a herb also included dosage information. Many of the monograph doses are for infusions or decoctions since this reflects the common use of teas in the German marketplace.11 Such daily doses are usually in the range of 2 to 10 g. Occasionally a monograph will specify a dose for a herb in terms of major active constituents; for example, for Ephedra the daily dose is 45 to 90 mg of alkaloids (about 4 to 8 g of herb) which is similar to the range in Table 6.1. Occasionally, where tincture and extract doses are given by the Commission E, there is not always a good correlation. For example, the single dose for valerian tincture is 1 to 3 mL and yet the single dose for a fluid extract is 2 to 3 mL. The reasons for this may be the same as those discussed above for the BHP 1983.
The Scientific Committee of ESCOP (European Scientific Cooperative of Phytotherapy) has published a series of herbal monographs.12,13 These were compiled by an international team of expert authors and represent a major contribution to the harmonisation of standards for herbal medicines across the European Union. These monographs contain useful dosage information reflecting the European situation and have been taken into account for the dosage recommendations in this text.
Clinical trials
The clinical trial is arguably the best way to determine the effective dose of either a single herb or a herbal formulation. This will not always be applicable to traditional medicine, however, since prescriptions are usually prepared on an individual basis. Also, a clinical trial does not necessarily determine the optimum dose. However, it does confer a relative certainty to the clinical results. That is, at a given dose of a given preparation a certain percentage of patients are likely to respond; for example, Ginkgo biloba standardised extract at 120 mg/day (which corresponds to about 6 g/day of dry leaves), given for 2 months, will improve intermittent claudication in 60% of patients.14
Sometimes the clinical trial has used a standardised extract of the herb which can then be correlated to the whole herb; for example, silymarin in liver disorders at 240 mg/day corresponds to 8 to 16 g/day of Silybum marianum seeds.15
The low dosage approach
In Europe, homeopaths often use combinations of herbal mother tinctures in drop dosage, for example, ‘drainage’. This approach is sometimes incorrectly labelled as ‘phytotherapy’.
In the USA a more direct influence comes, ironically, from a development of Eclectic medicine. In 1869, the Eclectic physician John Scudder proposed the concept of ‘specific medication’.7 With this concept, medicines were matched specifically to the symptom picture of the patient and then given in the minimum dose required. Although this system may seem similar to homeopathy, there were important differences.16 Material doses were always used, albeit lower than those prescribed by other Eclectics, and the prescription was not based on the law of similars. However, like classical homeopathy, there was a tendency to use only one medicine at a time.
Scudder initially proposed that ‘specific medicines’ should be tinctures prepared from the fresh plant.16 A fresh plant tincture is sometimes still called a ‘specific tincture’. Hence, the approach of using drop doses of tinctures, especially fresh plant tinctures, also comes from Scudder.
Although Scudder’s system of specific medication was seen as an important development in Eclectic medicine, it was considerably modified by Lloyd.17 Lloyd felt that drop doses of tinctures were too low and described the preparations proposed by Scudder as ‘superficial’. Lloyd proceeded to develop elaborate herbal preparations which were concentrated, semi-purified liquids. He also called these ‘specific medicines’ and they were widely adopted by Eclectic practitioners. However, in the early 20th century English herbalists aligned themselves with the American physiomedicalists in using simpler formulations, because Lloyd’s specific medicines proved too costly to import.
Lloyd sometimes used solvents other than ethanol and water in the preparation of his specific medicines.17 His methods were kept secret and even today are not widely known. Lloyd writes: ‘The aim has been to exclude colouring matters … and inert extractive substances also from these preparations …’. In this sense, he was tending towards the concept of orthodox drugs. However, his preparations were still chemically complex and ‘very characteristic’ of the original herb.17 According to Felter, the specific medicines developed by Lloyd were at least eight times stronger than 1:5 tinctures.7 It is these highly concentrated preparations which were generally used by Eclectic physicians in drop doses, and even then doses could be quite high – up to 60 drops (3 mL) three times daily.7
The current system in the UK
In the UK in the past herbalists used fluid extracts, usually prepared using heat or from concentrates. However, among newer practitioners in the 1980s there was disenchantment with these preparations because of their inconsistent quality. These practitioners instead adopted the use of 1:5 tinctures. Usually, formulations of tinctures are prescribed at doses of 2.5 to 5 mL three times daily. However, BHP 1983 doses for tinctures can only be achieved by this approach if the formulation contains one to three herbs (see Table 6.3 for examples). Unfortunately, this restriction is usually not followed and it can be concluded that the move to tinctures has resulted in the use of lower doses.
Oral dosage forms in herbal medicine
Liquids
Superior bioavailability is also an under-researched advantage of herbal liquids. When a solid dosage preparation is ingested, it must first disintegrate. The plant’s phytochemicals need to dissolve in digestive juices (and the water simultaneously imbibed with the tablet or capsule) in order to be absorbed by the body. Research has demonstrated that there is a relationship between the rate and degree of dissolution of the phytochemicals in a solid dosage preparation and their ultimate absorption into the bloodstream. The advantage of herbal liquids is that the all-important phytochemical constituents are already in solution.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


