Patient Story
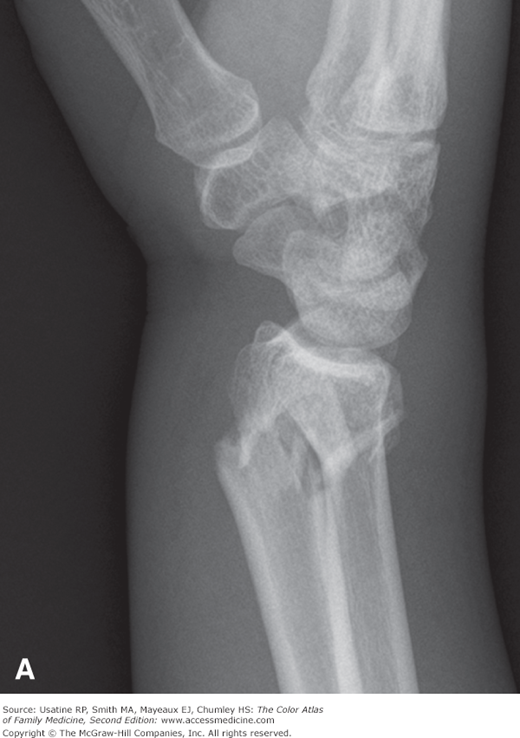
A 65-year-old woman tripped on a rug in her home and fell on her outstretched hand with her wrist dorsiflexed (extended). She felt immediate pain in her wrist and has difficulty in moving her wrist or hand. She has been postmenopausal for 15 years and has never taken hormone replacement therapy or bisphosphates. She presented with pain and swelling in her wrist. Her arm had a “dinner-fork” deformity. Radiographs showed a distal radius fracture with dorsal angulation on the lateral view (Figure 103-1).

Introduction
Synonyms
Epidemiology
- More common in older women—Female-to-male ratio of 3.2:1.1
- Prevalence—In a community study of 452 people older than age 40 years in the United Kingdom, 10.8% of women and 2.6% of men had a prior distal radius fracture.2
- Incidence—In Sweden, the incidence is 115 per 100,000 women and 29 per 100,000 men.1
Etiology and Pathophysiology
- Classic history is a fall on an outstretched hand.
- In patients older than 40 years of age, there is a strong association with osteoporosis. Patients with low-impact distal radius fractures have higher rates of osteoporosis than age-matched controls without fractures by bone density measured at the wrist (60% vs. 35%; p <0.001; odds ratio [OR], 5.7; 95% confidence interval [CI], 1.2 to 27.2) and lumbar spine (47% vs. 20%; p <0.005; OR, 3.9; 95% CI, 1.1 to 14.3).3
- Postmenopausal women and older men with distal radius fractures have an increased risk for a future hip fracture (relative risk [RR] = 1.53; 95% CI, 1.34 to 1.74; p <0.001; RR = 3.26; 95% CI, 2.08 to 5.11; p <0.001, respectively).4
Diagnosis
Diagnosis is suspected by a compatible history, such as falling on a dorsiflexed wrist and confirmed with a plain radiograph showing the fracture of the distal radius (Figure 103-1).
Patients present with wrist pain and are not able to use the wrist or hand. The distal radius typically angles dorsally, creating the “dinner-fork” deformity (Figure 103-1). Swelling is usually present.
Wrist radiographs (two views) confirm the fracture and demonstrate the degree of displacement and angulation.
While Colles fracture is the most common distal radius fracture, there are 3 other types that can be classified based upon their radiographic appearance, history and physical exam:
Smith fracture is a reverse Colles fracture in which the angulation is in the palmar direction. It usually occurs after a fall on a flexed wrist or a direct blow to the dorsal wrist. The distal radial metaphysis it is displaced and angulated in the palmar direction and an associated ulna styloid fracture may be seen (Figure 103-2).
Barton fracture is an intraarticular dorsal or volar rim fracture. It occurs with forced wrist dorsiflexion and pronation. A triangular fragment of the distal radial styloid occurs as seen in Figure 103-3.
Hutchinson fracture (chauffeur’s fracture) is a fracture through the base of the radial styloid. It occurs with forced hyperextension of the wrist. There will be tenderness at the radial styloid on exam and the radiograph indicates a radial styloid fracture (Figure 103-4). It is also named a chauffeur’s fracture from the past when a chauffeur would crank a car manually and the kick back could break the wrist in this pattern.

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


