Diffuse Large Cell Lymphoma
Key Facts
Etiology/Pathogenesis
May arise from progressive transformation of preexisting low-grade MALT lymphoma
Clinical Issues
Adults from 50-70 years of age
Usually peripheral in location
Microscopic Pathology
Sheets of large lymphoid cells with irregularly shaped, vesicular nuclei and prominent nucleoli
Areas of low-grade MALT-type lymphoma may be present focally
Tumors show a sharp interface with surrounding lung parenchyma
Can show variable cytomorphology depending on cell type involved
Diffuse large B-cell lymphoma
B-immunoblastic lymphoma
Anaplastic large cell lymphoma
Peripheral T-cell lymphoma
Ancillary Tests
Diffuse large B-cell lymphoma and B-immunoblastic lymphoma
Positive for CD20, CD79a, and kappa/lambda light chain restriction
Anaplastic large cell lymphoma (ALCL)
Strong paranuclear and membrane staining with CD30 and pan-T-cell antigens
Positivity for ALK1 in subset of cases
Peripheral T-cell lymphoma (PTCL)
Positive for pan-T-cell markers (CD3, CD45RO)
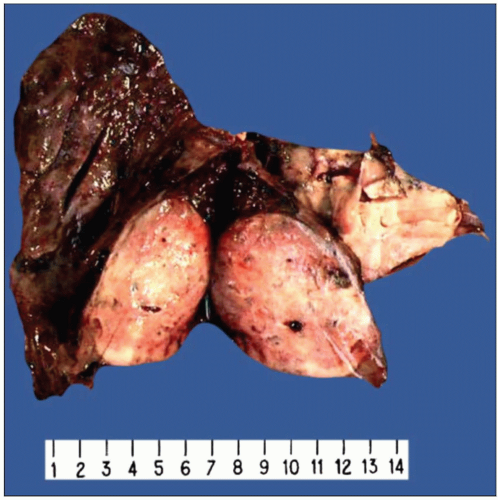 Gross appearance of diffuse large B-cell lymphoma of the lung on cut section shows a well-circumscribed tan-white nodule that is extensively replacing the lung parenchyma. |
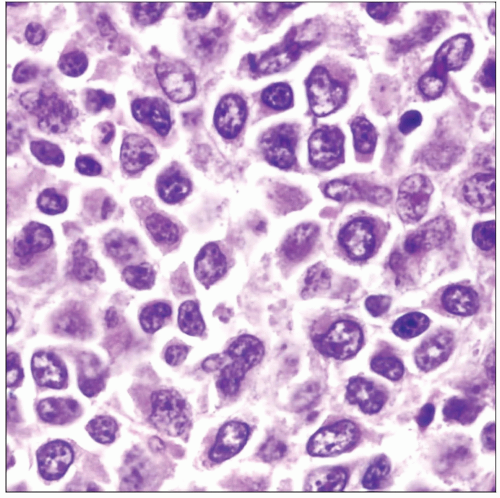 Histological appearance of diffuse large B-cell lymphoma of the lung shows a population of large lymphoid cells that are at least the same size as or larger than histiocytes. |
TERMINOLOGY
Abbreviations
Diffuse large cell lymphoma (DLCL)
Definitions
Diffuse proliferation of large lymphoid cells with nuclei exceeding the size of a normal macrophage
ETIOLOGY/PATHOGENESIS
Etiology
Can occur as complication of immunosuppression
May arise from progressive transformation of preexisting low-grade MALT lymphoma
CLINICAL ISSUES
Epidemiology
Incidence
Represents 10-20% of all pulmonary lymphomas
Age
Adults from 50-70 years of age
Site
Usually peripheral in location
Presentation
Cough
Dyspnea
Fever and night sweats
Treatment
Adjuvant therapy
Standard combination chemotherapy for DLCL
Prognosis
5-year survival with aggressive treatment has been reported in up to 60% of patients
IMAGE FINDINGS
Radiographic Findings
Chest x-rays show multiple or single opacity
MACROSCOPIC FEATURES
General Features
Well-circumscribed, tan-white tumor mass with rubbery cut surface
MICROSCOPIC PATHOLOGY
Histologic Features
Sheets of large lymphoid cells with irregularly shaped, vesicular nuclei and prominent nucleoli
Areas of low-grade MALT-type lymphoma may be present focally
Tumors show a sharp interface with surrounding lung parenchyma
Cytologic Features
Can show variable cytomorphology depending on cell type involved
Diffuse large B-cell lymphoma (DLBCL)
Large cells with enlarged nuclei displaying coarse chromatin pattern and prominent single nucleoli
Some tumors may show polylobated nuclei and multinucleated cells
Frequent mitotic figures & areas of tumor necrosis
Destruction of underlying structures and lung parenchyma
B-immunoblastic lymphoma (BIL)
Large nuclei containing single, large eosinophilic nucleoli, thick cell membranes, and abundant rim of cytoplasm
Destruction of underlying structures and lung parenchyma
Frequent areas of necrosis and high mitotic activity
Anaplastic large cell lymphoma (ALCL)
Most commonly of T-cell type (although a subset of ALCL may be of B-cell type)
Sheets of large, bizarre tumor cells with pleomorphic nuclei and abundant cytoplasm
Cells may resemble Reed-Sternberg cells or metastatic carcinoma cells
“Horseshoe” or kidney-shaped nuclei are characteristic of ALCL
Peripheral T-cell lymphoma (PTCL)
Admixture of large and medium-sized atypical lymphocytes with prominent nuclear convolutions and nuclear hyperchromasia
Hypervascularity and eosinophilic infiltration often accompany the tumor cell population
ANCILLARY TESTS
Immunohistochemistry
DLBCL and BIL
Tumor cells are positive for CD20 and CD79a and show kappa/lambda light chain restriction
ALCL
Strong paranuclear (Golgi zone) and membrane staining with CD30
Positivity of tumor cells for ALK1 in some cases
Positivity of tumor cells for pan-T-cell antigens (CD3, CD45RO)
Some cases may be positive for pan-B-cell antigens, such as CD20
PTCL
Positive for pan-T-cell markers (CD3, CD45RO)
Variable reactivity for CD2, CD5, and CD7
Molecular Genetics
Clonal gene rearrangements of immunoglobulin heavy chain can be demonstrated by PCR in DLBCL
Demonstration of t(2;5) chromosomal translocation in ALCL
Demonstration of clonal gene rearrangement of TCR genes in PTCL
DIFFERENTIAL DIAGNOSIS
Primary or Metastatic Poorly Differentiated/Anaplastic Carcinoma
Sheets of large atypical cells with discohesive growth pattern that can mimic ALCL
Positivity of tumor cells for epithelial markers (i.e., low molecular weight cytokeratins, EMA, MOC31)
Metastatic Malignant Melanoma
Sheets or nests of large, atypical tumor cells with prominent nucleoli and abundant cytoplasm
Tumor cells are strongly positive for S100 protein and other melanoma-associated markers (HMB45, Melan-A, tyrosinase)
Caveat: Melanoma cells can be positive for cytokeratins, CEA, and EMA in some cases
Lymphoepithelioma-like Carcinoma
Sheets of large atypical cells with scant cytoplasm and prominent nucleoli that can resemble DLCL
Syncytial growth pattern with dense stromal lymphoid cell infiltrates are characteristic
Strong positivity for cytokeratins and negative staining for lymphoid markers
Caveat: Some lymphoepithelioma-like carcinomas can be positive for CD30
SELECTED REFERENCES
1. Rush WL et al: Primary anaplastic large cell lymphoma of the lung: a clinicopathologic study of five patients. Mod Pathol. 13(12):1285-92, 2000
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


