10 Day surgery
Introduction
Summary Box 10.1 Clinical effectiveness of day surgery
• The surgical outcomes of a procedure performed on a day case basis or as an inpatient should, in theory, be identical, as it is the patient pathway and not the surgery that is different
• In practice, surgical outcomes from patients undergoing day surgery rather than inpatient surgery are often better as day surgery patients are a preselected cohort of healthier patients with fewer comorbidities.
Facilities for day surgery
Hospital integrated units
Summary Box 10.2 Cost effectiveness of day surgery
• Same-day admission and discharge avoids the costs of an overnight inpatient bed
• Criteria based pre-assessment reduce unnecessary investigations
• Dedicated day or ambulatory theatre lists maximize surgical throughput
• Protocol-based discharge with comprehensive patient information reduces unplanned hospital readmissions.
The patient pathway
First patient contact
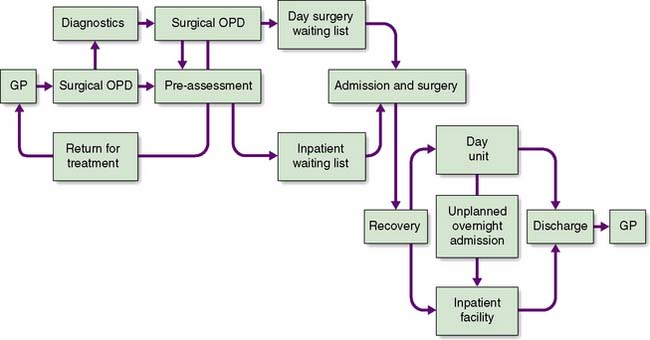
An efficient and effective ambulatory pathway (Fig. 10.1) requires the patient to arrive at the day unit on the day of surgery fully prepared for their procedure both physically and mentally. Preparation for possible day surgery starts at first patient contact with their General Practitioner. Patients will often raise the topic of day surgery themselves as their preferred management option at their initial consultation. A brief ‘health screen’ with the GP referral letter detailing the patient’s blood pressure, body mass index, medication and past medical history allows the surgeon at out-patients to consider appropriate pre-assessment required for the patient. If no diagnostic or other investigations are required, the patient can be listed for their surgical procedure and referred immediately for pre-assessment, avoiding a follow-up out-patient clinic appointment.
ASA status
This is used to assess the physical state of the patient prior to surgery and has been adopted worldwide (Table 10.1). Most day units accept ASA I and II patients. More advanced units and those that can deal safely with unplanned overnight admissions may accept some patients with ASA III status such as insulin-dependent diabetics.
Table 10.1 American Society of Anaesthesiologists classification of physical status
| ASA I | Normal healthy patients. Little or no risk for surgery. |
| ASA II | Patients with mild systemic disease. Minimal risk during treatment. Examples include well-controlled non-insulin dependent diabetes, mild hypertension, epilepsy or asthma. |
| ASA III | Patients with severe systemic disease that limits activity but is not incapacitating. These patients need medical input before surgery. Examples include insulin-dependent diabetes or a history of myocardial infarction, congestive heart failure or cerebrovascular accident in the preceding six months. |
| ASA IV | Patients with severe systemic disease limiting activity and is a constant threat to life. Elective surgery is contradicted and emergency surgery requires urgent medical input. Examples include unstable diabetes, hypertension and epilepsy or a recent myocardial infarction. |
| ASA V | Patients who are moribund and not expected to survive more than 24 hours without an operation |
Pre-assessment
Pre-assessment is offered to the patient in a number of options:
1. At source in the GP surgery. This model is used in surgical outreach clinics when the pre-assessment nurse accompanies the surgeon to the clinic. It is more cost effective however to train a practice nurse to perform the routine pre-assessments and refer more complex patients for hospital pre-assessment.
2. At the pre-assessment clinic. Formal pre-assessment consultations can be programmed in advance for 30–60 minute interviews depending on the complexity of the patient.
3. At the surgical outpatient clinic. Where a number of surgical clinics are running concurrently, it is cost effective to offer patients a ‘one-stop’ pre-assessment service. Patients requiring more complex pre-assessment can be deferred to a planned pre-assessment clinic at a later date.
4. By telephone, postal questionnaire or internet (e-mail or on-line). This model is suitable for fit patients undergoing straightforward procedures especially if they have already had a basic health screen performed at the GP surgery.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


