Darier Disease
Irina Margaritescu, MD, DipRCPath
Key Facts
Etiology/Pathogenesis
Autosomal dominant genodermatosis
Mutations in gene ATP2A2
New mutations in ˜ 25% of cases
Clinical Issues
Age
Typical onset in late childhood or adolescence
Presentation
Symmetrical, greasy, crusted, keratotic, yellow-brown itchy papules and plaques on seborrheic areas
Longitudinal nail streaks and nail splitting with V-shaped notch at distal margin
White papules with cobblestone appearance on buccal mucosa
Microscopic Pathology
Several discrete foci of suprabasal clefts with acantholytic dyskeratotic cells surmounted by vertically oriented parakeratotic columns
Little, if any, inflammatory cell infiltrate
Top Differential Diagnoses
Hailey-Hailey disease
Galli-Galli disease
Grover disease
Diagnostic Checklist
Focal acantholytic dyskeratosis that typifies Darier disease represents a histological reaction pattern and is not specific for this condition
Clinicopathological correlation is essential
 Photograph shows typical clinical features of Darier disease, namely greasy, crusted, keratotic, yellow-brown papules and plaques on seborrheic areas. |
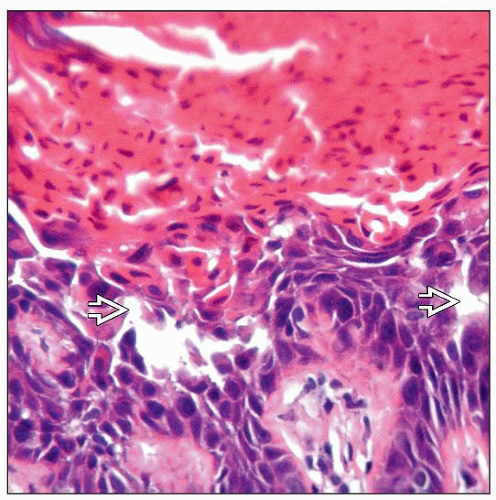 The histological hallmark of Darier disease is focal acantholytic dyskeratosis  . . |
TERMINOLOGY
Abbreviations
Darier disease (DD)
Synonyms
Darier-White disease, keratosis follicularis
Definitions
Autosomal dominant genodermatosis characterized clinically by greasy hyperkeratotic papules in seborrheic regions, nail abnormalities, and mucous membrane changes and histopathologically by acantholysis and dyskeratosis
ETIOLOGY/PATHOGENESIS
Etiology
Mutations in gene ATP2A2
Located on 12q23-24.1
Encodes sarcoplasmic/endoplasmic reticulum Ca2+-ATPase isoform 2 protein (SERCA2)
> 113 familial and sporadic mutations identified
New mutations in ˜ 25% of cases
Pathophysiology
SERCA2 maintains low cytoplasmic Ca2+ level by transporting calcium ions from cytosol into lumen of endoplasmic reticulum
SERCA2 mutations cause alterations in cytosolic Ca2+ homeostasis that result in
Dyskeratosis due to reduced expression of antiapoptotic proteins Bcl-2, Bcl-x, and BAX
Acantholysis due to impaired trafficking of desmoplakin and abnormal desmosomal assembly
Heat, sweat, humidity, sunlight, UVB exposure, lithium, oral corticosteroids, mechanical trauma, and menstruation can exacerbate disease
UVB downregulates ATP2A2/SERCA2 expression via induction of COX-2 expression and subsequent increase of PGE(2) production in keratinocytes
CLINICAL ISSUES
Epidemiology
Incidence
4 new cases per 1 million over 10 years
Age
Typical onset in late childhood or adolescence
As early as age 4
Case of congenital keratosis follicularis reported
Gender
Males and females equally affected
Ethnicity
Worldwide distribution
Site
Seborrheic areas such as forehead, temples, ears, nasolabial folds, scalp, upper chest, and back
Flexural areas including axillae, inframammary fold, groin, and perineum
Hands and nails
Mouth, anogenital mucosa, and sometimes pharynx, larynx, and esophagus
Presentation
Symmetrical, greasy, crusted, keratotic, yellow-brown itchy papules and plaques
Flexural malodorous, hypertrophic, and vegetative plaques
Acrokeratosis verruciformis-like lesions on dorsum of hands and feet
Palmar pits
Longitudinal white &/or red nail streaks, subungual hyperkeratosis, longitudinal nail splitting with V-shaped notch at distal margin
White papules with cobblestone appearance on mucosa of cheeks, palate, and gums
Other clinical variants include hypertrophic, vesiculo-bullous, comedonal, hemorrhagic, linear, or segmental types
Neuropsychiatric abnormalities including epilepsy, bipolar disorder, and mental retardation have been described in some cases
Laboratory Tests
Gene sequencing can be used to confirm diagnosis



